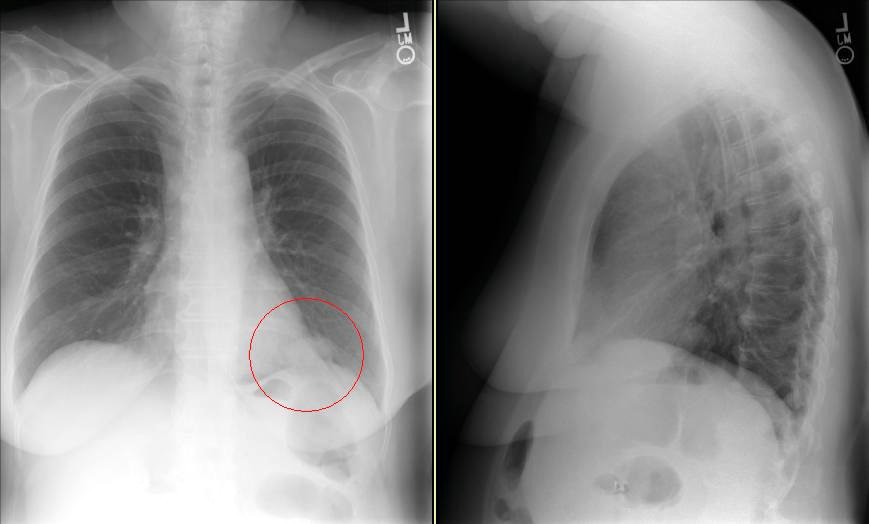
This patient came to me pre-worked up so I will show all the data she had had thus far. This is a 65 y/o woman with no TOB Hx, normal PFTs who had a persistent cough. She had an abnormal CxR (see above) and here PCP ordered a CT and then a PET-CT and she was sent to us.
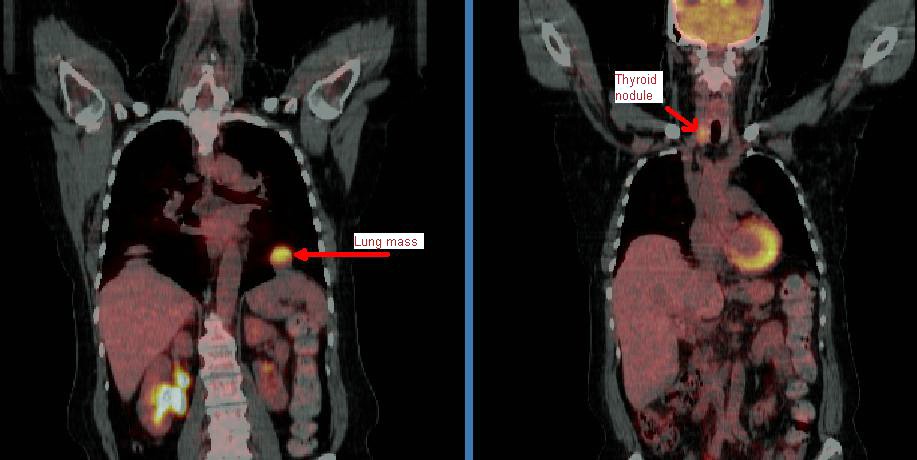
Her PET scan showed two very FDG-avid lesions. A L basilar lung lesion and a R thyroid nodule with no other abnormal uptake. She is euthyroid clinically and by TFTs.
Do you think the lesion are related?
Would you biopsy one, the other, both?
I had a very similar consult recently, except the patient had severe COPD (FEV1 0.7) and a large nodule abutting the chest wall. I recommended starting with a biopsy of the thyroid to avoid the risk of a PTX. Path came back suggestive of papillary ca, but they couldn't call it. Ended up biopsing the nodule, after which the stains suggested the thyroid was a metastatic lesion from the lung primary (mucinous adeno).
ReplyDeleteI think anaplastic thryoid ca's are the most likely to spread to the lung, but I've heard the thyroid lesions should be pretty large by that point.
Cool case: What does the thyroid lesion look like on the transmission CT images? A recent Journal of Nuc Med article looked at this: If the lseion appears primarily cystic, it is very unlikely to be cancer.
ReplyDeleteProbably best to bx the Thyroid first otherwise. This case could easily represent 2 sepearate primaries.