We were asked to see this 74 y/o woman for dyspnea and atypical chest pain. She has a long TOB Hx (>50 p/y) and continues to smoke. Last year she had a "lump" in her neck (it was benign) and had an unremarkable neck and chest CT scan. For the past 2 weeks she has had worsening dyspnea and a cough productive of blood-streaked clear sputum.
No othe significant PMHx or exposures.
Her exam reveals decreased BS on the L with faint crackles and her CxR is seen below:
What would you do next?
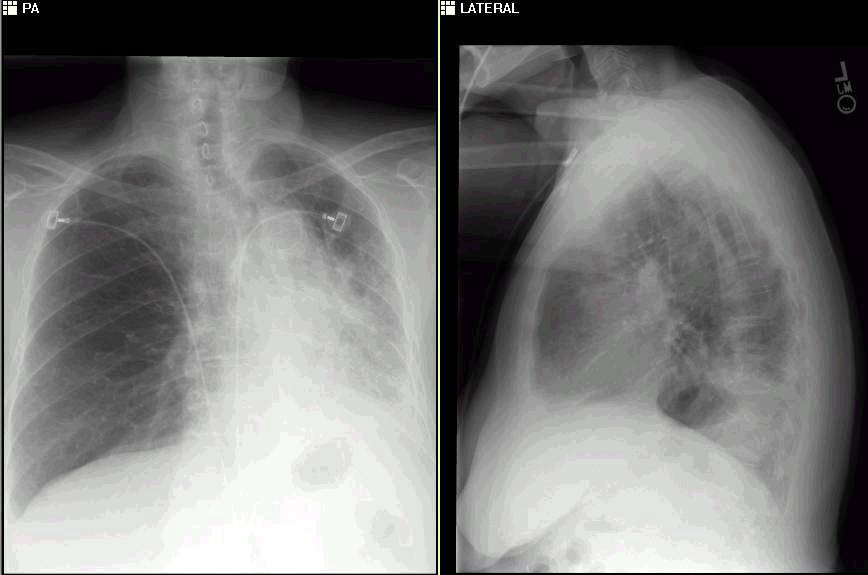
The resolution on my monitor is poor, but it looks like you have a LLL posterior lesion with tracheal deviation to the left. I MAY see the sudden cuttoff of the left lower lobe bronchus (just below the mainstem), but I cannot be sure if it is artifact.
ReplyDeleteI would be worried about an endobronchial lesion causing lobar atelectasis.
She needs a CT scan, I would send sputum cytology if she is coughing anything up.
Ultimately, a bronch would probably be necessary
Any surprise that he had an unremarkable CT of chest less than a year ago?
ReplyDeleteMake it 3 for 3. Volume loss on the left with shift, suspicious for an endobronchial lesion. I'd do a CT scan to eval for lymphadenopathy, the bronch +/- Wang.
ReplyDeleteI will post the CT and some f/up tomorrow to allow for more comments.
ReplyDelete