He was admitted to the ICU with hypoxemic respiratory failure requiring intubation for what turned out to be herpes pneumonitis, and was treated with a 21 day course of acyclovir. Over this course, he was easily ventilated and oxygenated with progressively improving respiratory parameters. On two occasions, his weaning parameters were excellent, and he easily tolerated minimal ventilatory support (PS-5/PEEP 5) for 2 hours. Each time, he required re-intubation for respiratory distress several hours after extubation.
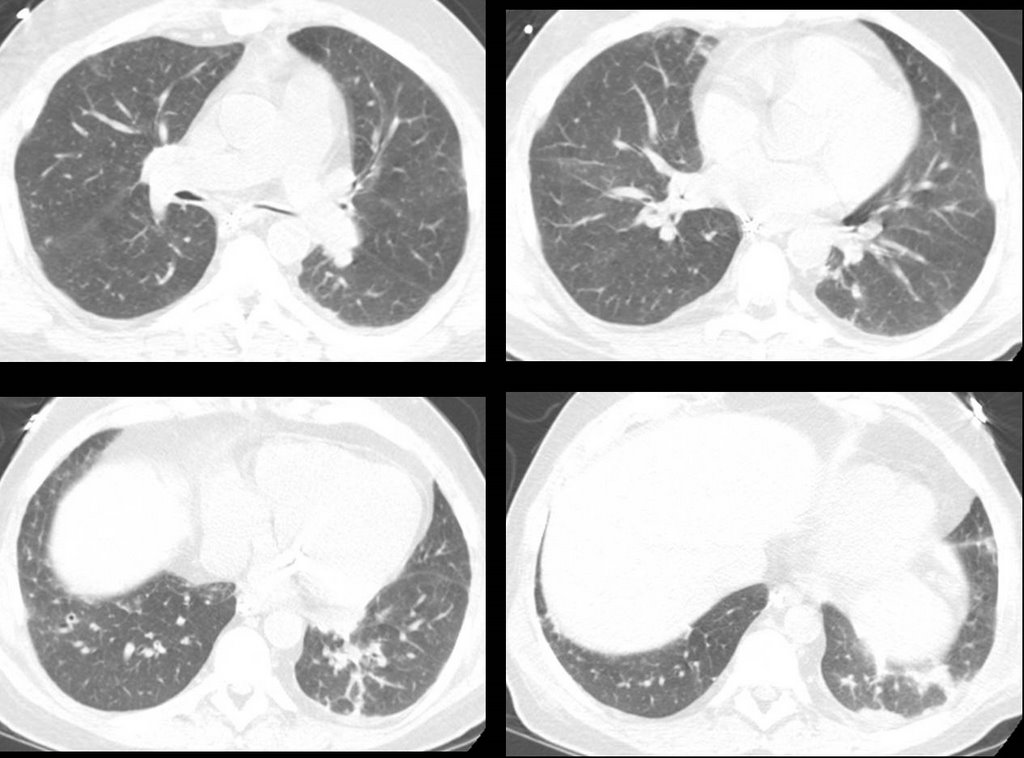
Here's some representative cuts from a CT scan done about 10 days into his hospital course.

2 comments - CLICK HERE to read & add your own!:
Those are great films, Jeff! How is he doing now?
The CT was actually done while the patient was intubated AND on positive pressure ventilation. On bronchoscopy, there was severe, diffuse, tracheobronchomalacia, which I thought explained his inability to maintain ventilation when extubated.
He has since had a tracheostomy placed, and a stent has been put in the left mainstem bronchus. The hope is for staged-placement of multiple tracheal and bronchial stents--we don't know if they will work, but if they don't he'll need chronic positive pressure ventilation.
As to the etiology, this topic was recently reviewed in (CHEST 2005; 127:984–1005). Best guess is chronic inflammation due to recurrent tracheobronchitis, although we just don't know.
Post a Commenttest post a comment