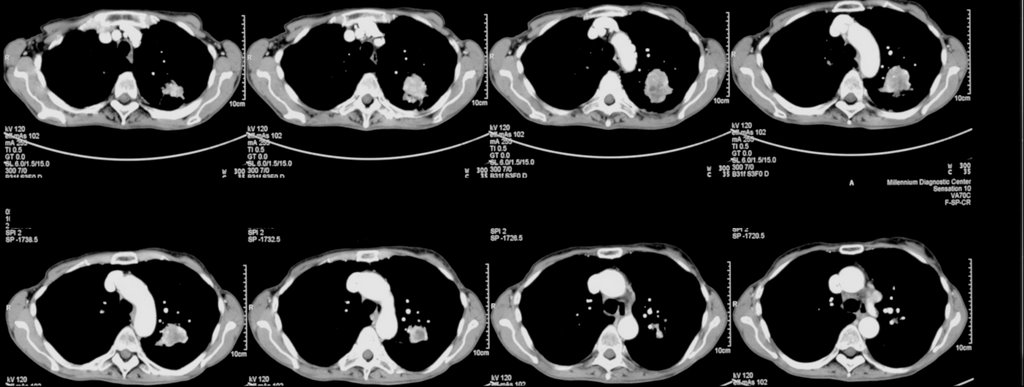
70 year old woman with COPD FEV1 34% predicted, but she is well compensated and on no supplemental oxygen (91% on RA). A LUL lesion was noted (see below) and workup included 2 bronchs (one with ultrasound-guided) and 1 CT-guided biopsy. All were negative for malignant cells. BAL was not done but Tbbx showed Atypical lymphoid cell with acute inflammation and Filamentous bacteria. BAL was not sent so we don't have micro ID (the bacteria was identified by path).
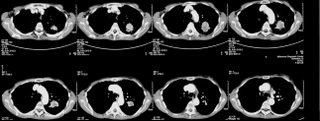
Cancer is obviously still number one on the list, but I dont think she's a surgical candidate and in terms of treating with chemo, we still dont have a tissue diagnosis. On the other hand, the filamentous bacteria finding is interesting. What is your impression and what would you all do next? Thanks.
5 comments - CLICK HERE to read & add your own!:
Sounds like actino to me. Start amoxicillin and repeat CT in 6 weeks.
Do you think she could tolerate a wedge?
She's not a surgical candidate it turns out (no surprise). I want to treat the "filamentous" bacteria. How would you treat this, given that you can't differentiate between actino and nocardia? Would anyone give both PCN and bactrim?
Nocardia is weakly AFB and usually disease of an immunocompromised host.
Agree with PET. It may help you find another lesion. It would also help you nuclear radiologist (ie me) find a VERY metabolically acitve part of the lesion to biopsy. I tend to target the hottest part of the lesion....and it seems to help my results. I would also do a core biopsy of this (although the smallest core needle they make)
Post a Commenttest post a comment