I had posted on this
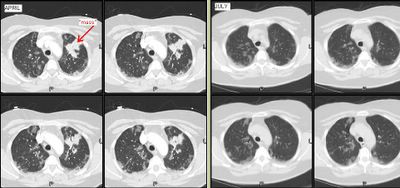
59 y/o woman with a funny presentation: she had had an episode of syncope at home, hit her head and had a skin lac requiring 7 stitches. While being worked up in the ER they found her to be hypotensive and febrile with an abnormal CxR and CT of the chest. She had MSSA in her sputum and a dense lung "mass". I bronch'ed her and got "organizing pneumonia" but no malignancy. She got ABTx and the "mass" went away completely. She did however had persistent smallish alveolar infiltrates seen below:
I re-bronched her focusing on the infiltrates since they had persisted for 3 months after the initial presentation. She had a lot of eosinophilic proteinaceous alveolar material and our pathologists sent the tissue to T. Colby who thought this was PAP.
Would you be satisfied with this Dx on TBBx or would you pursue an OLBx?
How about testing for anti-GM-CSF Antibodies?
She has almost normal lung function, how would you treat her?

1 comments - CLICK HERE to read & add your own!:
Well, anti-GM-CSF antibodies could be detected but only if it was primary PAP. If the PAP was secondary to another condition, the ab's would not be high. In 1 study, the AB were positive in both blood and BAL fluid samples in 12 of 13 primary (idiopathic)PAP patients but in noe with secondary or normal subjects. Thorax 2006;61:528-534
Post a Commenttest post a comment