This is a 38 year old man who is 1.5 years s/p a bone marrow transplant for non-Hodgekin's Lymphoma that had relapsed despite several chemotherapeutic regimens. His post-transplant course has been generally uneventful, with good engraftment, no major infectious complications, and minimal GVHD of the skin and gut. He also had a DVT at some point, treated with adequate anticoagulation for 9 months. He was referred for a right pleural effusion. This was tapped-it was a chylothorax. Flow-cytometry was negative for a recurrence of the lymphoma.
His pulmonary function varies a bit between normal and a mild obstructive ventilatory defect. His exercise capacity has continued to improve since the BMT, but remains significantly below his pre-morbid state (he was, prior to his cancer, a highly trained endurance athlete).
He is referred for pleuradesis.
His films are below:
His pre-BMT film:

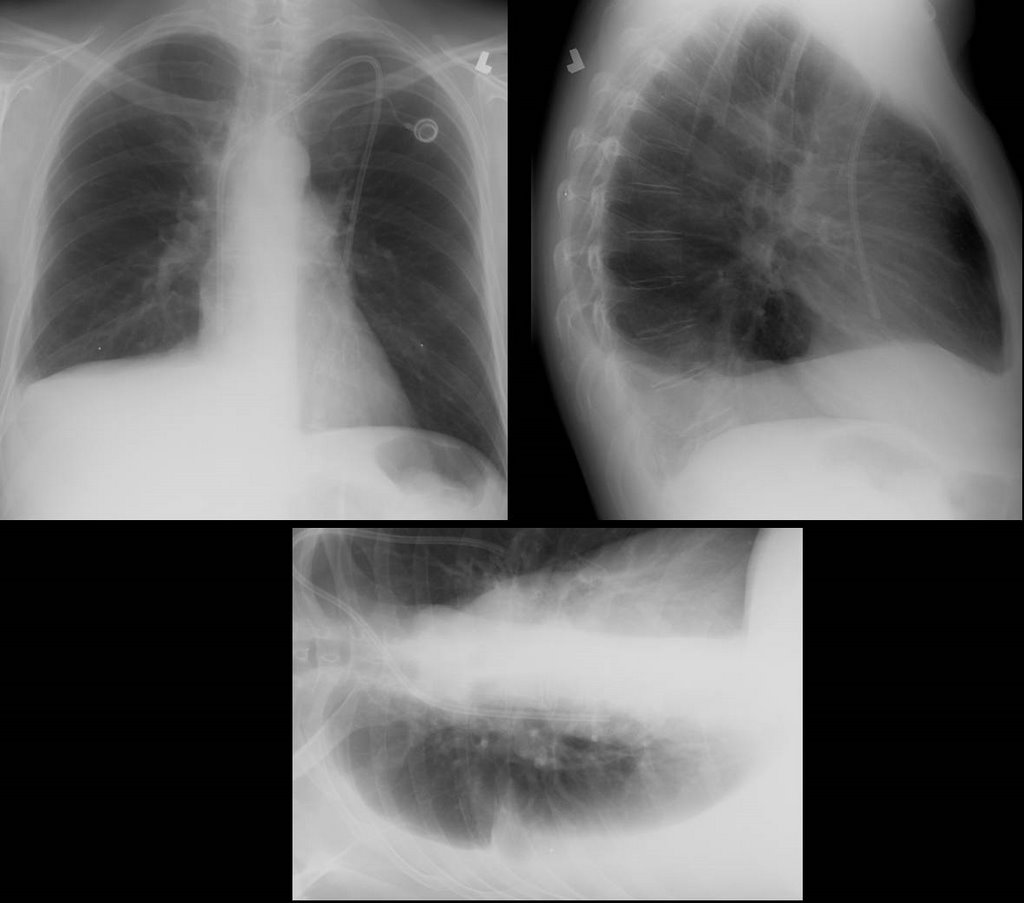
One year later, prior to thoracentesis:

One-day following a 2-liter thoracentesis

Thoughts? How would you proceed?


5 comments - CLICK HERE to read & add your own!:
Well, the presence of the cylothorax would make me worried that the lymphoma is back and is compressing thoracic duct. I would start with CT of chest to look specifically at this question.
Several CT scans of the chest only showed the effusion, without any enlarged nodes to suggest recurrence of the lymphoma. The parenchyma was normal.
This is really a management question: assume that the effusion is a benign chylothorax resulting from damage to the thoracic duct due to the initial lymphoma or from the thoracic radiation given to treat it. The question is: how would you treat it? Would you treat it? And, specifically, would you proceed with pleurodesis as requested by the referring hematologists?
One of the possible problems of chest tube pleurodesis with a chylothorax is the constant output which "washes out" the talc and can continue for a while and even lead to nutrition problems.
Not much interest, so I'll just wrap it up. I posted this to highlight the fact that the effusion really has not changed in the year and a half since the bone marrow transplant. Although it reamains free flowing, the lack of significant change following a large volume thoracentesis suggests that it is accumulating rapidly. So, I think the liklihood of complete drainage allowing for a successful surgical or medical pleurodesis is low, and would not recommend it. I agree with the post regarding nutritional problems, as chest-tube drainage of a reaccumulating chylothorax definitely poses that risk.
So: 1) I do not think the effusion is causing significant impairment in pulmonary function,
2) I think the effusion is stable and rapidly reaccumulates following drainage
3) I would not recommend pleurodesis for this patient.
4) Should the effusion pose a significant problem in the future, I think that surgery to attemt to bypass or repair the thoracic duct would be the "best" option...
I agree that surgical would be the way to go if one decided to pleurodese the patient. With a rapidly reaccumulating chyloTx medical (i.e. chest tube) pleurodesis would not work well. You would need (as noted in a previous post) to basically keep the patient in the hospital on a essentially-fat-free diet and hope tha talc would "take" after a few instillations.
Post a Commenttest post a comment