lymphopenia, and some alopecia. She also has leukopenia.
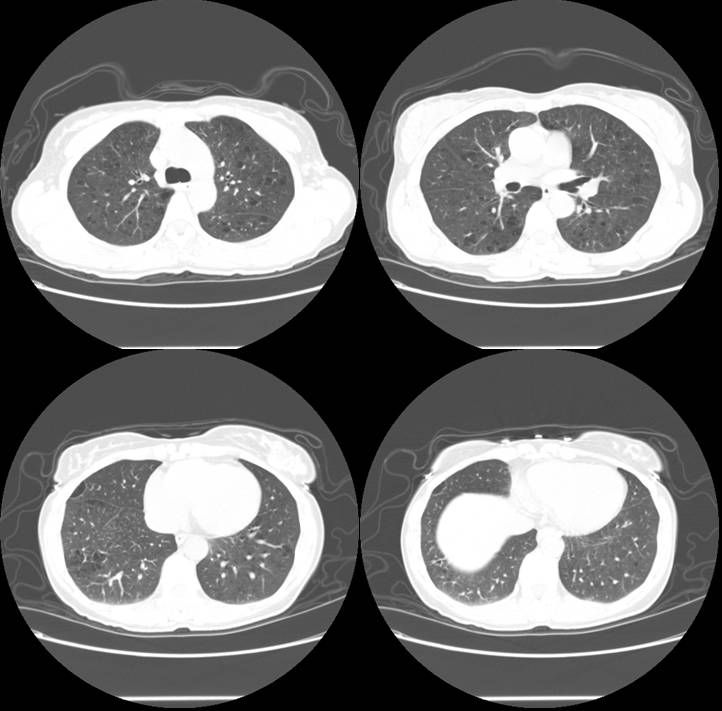
She has no respiratory symnptoms. A routine CXR followed by a high res CT are shown below.


A bronchoscopy was done. Tbbx of the upper lobe revealed (path report):
very mild chronic inflammation and intra-alveolar hemosiderin laden macrophages. These findings are non-specific. Also present is a fragment of epithelium and scant fibrous stroma with a papillary configuration.
Any thoughts?
5 comments - CLICK HERE to read & add your own!:
So, it looks like these cystic lesions are present in both the upper and lower lobes bilaterally. Setting aside the Lupus for a moment, these thin wall cysts raise suspicion for Langerhan's cell histiocytosis/eosinophilic granulama, LAM, or an atypical appearence of sarcoid. A did a quick search and did not find any known association between these diseases and Lupus (and the diagnosis of Lupus here seems pretty well established).
I did find one report of Lymphocytic interstitial pneumonitis (LIP) and diffuse think wall cysts in a patient with SLE.
Finally, is this patient being treated with immunosupression for the Lupus. We need to consider atypical infections, and in light of the multiple diffuse cysts, I would have to consider PCP, although I would have expected this to be found on a BAL.
Bottom line: in the absence of a definitive diagnosis here, I would probably proceed with a surgical biopsy.
good comments; BAL: micro all negative (including PCP). The cell count was 117 WBC's with 97% macrophages. We sent off a CD1a but didn't see it in the computer. Iguess the biopsy is too small to rule out an LIP, as you suggest. I agree with open lung as next step now that infection is pretty much ruled out.
I did a search and seem to remember lupus can have cysts in lung but can't remember where I saw that so who knows.
As for LAM, the HMB-45 stain was negative.
Lupus and Sjogren's can also present with bronchiectasis but i haven't found an association with cysts like those either. Is she a smoker?
What do her PFTs look like?
The patient quit smoking 5 years ago. She used to smoke 15 cigarettes a day for 12 years. Her PFT's are normal (120% predicted) but her DLCO is slightly decreased at 71% predicted.
Post a Commenttest post a comment