A 70 year old man has reactive airways dysfunction syndrome from a previous inhalant. He was seen in 2005 for dyspnea but primary did not initiate any steroids. At that time his fev1 was 2.05, 66% predicted. When we saw him in January where there was obstruction with an FEV1 of 2.34 (72% predicted). 20 mg of steroids were given (higher doses resulted in his fingers "locking") and a repeat spiro this month shows no change in the obstruction (2.27 l, 69% predicted).
How many would continue the steroids? How many would stop the steroids for apparent lack of efficacy?
Symptomatically he has mild dyspnea with exertion that is less than prior to the steroids.
Showing posts with label asthma. Show all posts
Showing posts with label asthma. Show all posts
Tuesday, March 20, 2007
Tuesday, November 07, 2006
ICS in the hospital
What is your usual practice regarding inhaled steroids when you admit a patient for either status asthmaticus or AECB?
If they are already on an ICS on admission and they will be on a systemic steroid do you continue the ICS?
Conversely, if they are not on an ICS on admission and are now on a systemic steroid, do you start an ICS during the admission or after D/C?
If they are already on an ICS on admission and they will be on a systemic steroid do you continue the ICS?
Conversely, if they are not on an ICS on admission and are now on a systemic steroid, do you start an ICS during the admission or after D/C?
Tuesday, September 05, 2006
Pulmonologist with high IgE
At ATS there was a stand on a rapid IgE testing system on capillary blood and some of us had it done just to check out the system.
One of us (with Hx of rhinitis but noasthma) had the results come back at an IgE level of 900 (their upper limit was 136).
Would you investigate it any further (CBC with diff, etc.) ?
One of us (with Hx of rhinitis but noasthma) had the results come back at an IgE level of 900 (their upper limit was 136).
Would you investigate it any further (CBC with diff, etc.) ?
Thursday, August 24, 2006
Prune-belly
I have just seen a 26 y/o patient in the office for recurrent respiratory tract infections. He has a Hx of prune-belly syndrome (poor abdominal muscle development with severe urinary tract abnormalities) and has been on HD after a failed renal Txp.
These patients tend to have a restrictive physiology because of the oligohydramnios and sometimes even have hypoplastic lung. Indeed his TLC is ~66%. His Cxr is pretty unremarkable but he also has an associated obstructive defect: FEV1 is ~36% witha ratio of<70%. Has anybody seen this condition (or similar ones) be associated with asthma/reactive airways disease?
These patients tend to have a restrictive physiology because of the oligohydramnios and sometimes even have hypoplastic lung. Indeed his TLC is ~66%. His Cxr is pretty unremarkable but he also has an associated obstructive defect: FEV1 is ~36% witha ratio of<70%. Has anybody seen this condition (or similar ones) be associated with asthma/reactive airways disease?
Wednesday, July 05, 2006
Obesity and obstructive lung disease
I see a lot of obese patients with mild to moderate obstruction on PFTs without smoking Hx or a clear Hx of asthma and atopy (TN has a state average BMI of 29). There was an ATS session on obesity and airways disease and a lot of interest on this correlation at NIH.
Did any of you attend the symposia on this topic? Would you manage this obstruction in a different way for this patients?
Did any of you attend the symposia on this topic? Would you manage this obstruction in a different way for this patients?
Tuesday, June 20, 2006
Asthma and IgE
I saw this 50 y/o man with a label of remote asthma who had quit smoking in 1980 for cough, wheezing and dyspnea. He gave a good Hx for asthma and had an FEV1 of 58% with FVC: 65%, normal TLC and normal DLCO. I started treatment and a few months later on ICS his FEV1 had come up to 69% but he still had a significant cough. In searching for triggers (e.g. GERD) and other conditions (e.g. ABPA) I found an IgE level of 927 (upper limit 158). Since he was still wheezing I gave him some prednisone and continued the ICS. His FEV1 is now 73% and he feels better. His IgE is now 655.
Would you bother following the IgE at all?
Since he still has a persistent (mild) defect, would you give him any more systemic steroids?
Have you had a good experience with Xolair?
Would you bother following the IgE at all?
Since he still has a persistent (mild) defect, would you give him any more systemic steroids?
Have you had a good experience with Xolair?
Monday, June 19, 2006
A "simple" question
Ok, I just had my first patient call and ask to be taken off of Advair because of the recent press regarding the "risk" of death associated with long-acting beta-agonists. See the following editorial:
Martinez FD, NEJM December 22, 2005
and the recent meta-analysis:
Salpeter SR, Ann Int Med, June 20, 2006
Here's a figure from the Salpeter paper:
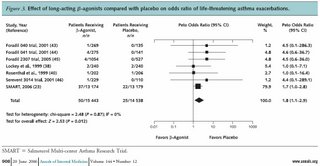
Our goal here is not to turn the blog into a journal club, but I think this has important implications on both practice and liability. Am I the only one who thinks that while the "relative" risk is increased, the "absolute" increased risk is amazingly small. I'm not sure that the increased "risk" outweighs the benefits of LABA's in patients with moderate or severe persistent asthma, or in patients with COPD who remain symptomatic despite anticholinergics.
So, I'm interested to hear how the pulmonary community is approaching these data...
Martinez FD, NEJM December 22, 2005
and the recent meta-analysis:
Salpeter SR, Ann Int Med, June 20, 2006
Here's a figure from the Salpeter paper:

Our goal here is not to turn the blog into a journal club, but I think this has important implications on both practice and liability. Am I the only one who thinks that while the "relative" risk is increased, the "absolute" increased risk is amazingly small. I'm not sure that the increased "risk" outweighs the benefits of LABA's in patients with moderate or severe persistent asthma, or in patients with COPD who remain symptomatic despite anticholinergics.
So, I'm interested to hear how the pulmonary community is approaching these data...
Tuesday, May 02, 2006
Exercise-induced asthma
What's the best way to diagnose exercise-induced asthma in a patient where the history seems to fit and baseline spiro is negative: methacholine challenge or post-exercise spirometries?
Thursday, February 16, 2006
Progressive Disease?
Quick case: a 55 year old woman was diagnosed with Sarcoidosis in 2000 based on a biopsy of a skin lesion. At the time, she was referred to my institution where saw a young, but talented fellow (CEOB). She had mild bilateral hilar adenopathy and some atypical diffuse interstitial markings. The biopsy was reviewed and the diagnosis confirmed. She has never received any treatment for sarcoidosis, and her pulmonary function remained normal for 4-5 years.
Co-morbidities include: asthma and fibromyalgia.
I began seeing her about year ago (after a second fellow who took over many of CEOB's patients). The first time I saw her, she had a new complaint of persistent chest tightness and a marked decline in her pulmonary function: DLCO decreased from a stable baseline of 77% to 60%. FEV1 and FVC dropped from 82% and 86% of predicted values to 72% and 74% respectively.
She was started on an inhaled corticosteroid and long acting beta-agonist, and we ordered a HRCT: I don't have the images, but compared to a CT done 2 years previously, there was:
1. Progressive areas of scarring/fibrosis in the lingula, middle
lobe, and right upper lobe, the latter associated with atelectasis.
2. Increasing parenchymal nodules, predominantly in the left upper lobe.
3. Stable mediastinal and upper abdominal lymph nodes.
We discussed bronchoscopy and immunosupressive therapy for treatment of sarcoidosis, but she was very resistant to therapy and we chose a "watchful waiting approach."
In follow-up (after 3 and 6 months), she has had consistent improvement in her pulmonary function, so that her FEV1, FVC, and DLCO are now the same (or better) as they were in 2000. She continues to complain of some persistent chest tightness, but otherwise feels much better and is not limited in any activity.
So, here are the clinical questions:
1)Would one treat for radiographic progression of Stage 4 sarcoidosis in the absence of a decline in pulmonary function?
2)Do you think that the persistent "band-like" chest tightness is related to either her sarcoidosis or to asthma?
Co-morbidities include: asthma and fibromyalgia.
I began seeing her about year ago (after a second fellow who took over many of CEOB's patients). The first time I saw her, she had a new complaint of persistent chest tightness and a marked decline in her pulmonary function: DLCO decreased from a stable baseline of 77% to 60%. FEV1 and FVC dropped from 82% and 86% of predicted values to 72% and 74% respectively.
She was started on an inhaled corticosteroid and long acting beta-agonist, and we ordered a HRCT: I don't have the images, but compared to a CT done 2 years previously, there was:
1. Progressive areas of scarring/fibrosis in the lingula, middle
lobe, and right upper lobe, the latter associated with atelectasis.
2. Increasing parenchymal nodules, predominantly in the left upper lobe.
3. Stable mediastinal and upper abdominal lymph nodes.
We discussed bronchoscopy and immunosupressive therapy for treatment of sarcoidosis, but she was very resistant to therapy and we chose a "watchful waiting approach."
In follow-up (after 3 and 6 months), she has had consistent improvement in her pulmonary function, so that her FEV1, FVC, and DLCO are now the same (or better) as they were in 2000. She continues to complain of some persistent chest tightness, but otherwise feels much better and is not limited in any activity.
So, here are the clinical questions:
1)Would one treat for radiographic progression of Stage 4 sarcoidosis in the absence of a decline in pulmonary function?
2)Do you think that the persistent "band-like" chest tightness is related to either her sarcoidosis or to asthma?
Subscribe to:
Posts (Atom)