One of my patients has had persistent post-thoracotomy pain following a RULobectomy in 9/05. She has been on gabapentin and narcotics; tried nerve root blocks (with short-lived results) and is not a drug-seeker. She has now undergone a dorsal rhizotomy (confirmed by path of the dorsal root ganglion) and after a 1-week improvement is now having even more pain.
What do you usually do for these cases of persistent post-thoracotomy pain that extend for months and years?
Showing posts with label surgical. Show all posts
Showing posts with label surgical. Show all posts
Tuesday, January 02, 2007
Tuesday, November 21, 2006
CXR followup after resection
A curious reader from Maine would like to know:
How frequently and for how long, do you follow xray/CT's after the surgical resection of a stage 2 lung cancer.
How frequently and for how long, do you follow xray/CT's after the surgical resection of a stage 2 lung cancer.
Friday, November 03, 2006
preop stage
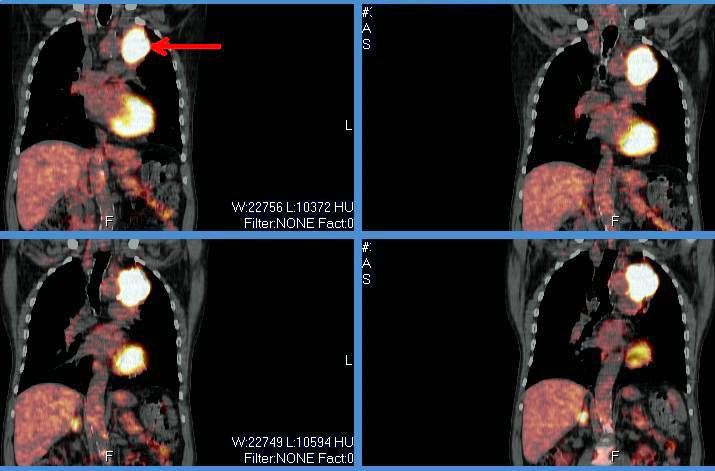
I thought this was an interesting case because it involves role and possible limitations of PET scanning for staging prior to surgical resection. A 69 year old presented with a LUL mass. The bronch brushings revealed non-small cell lung cancer. A PET showed the intense uptake in that mass:
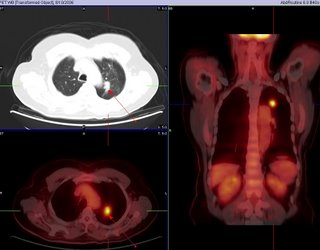
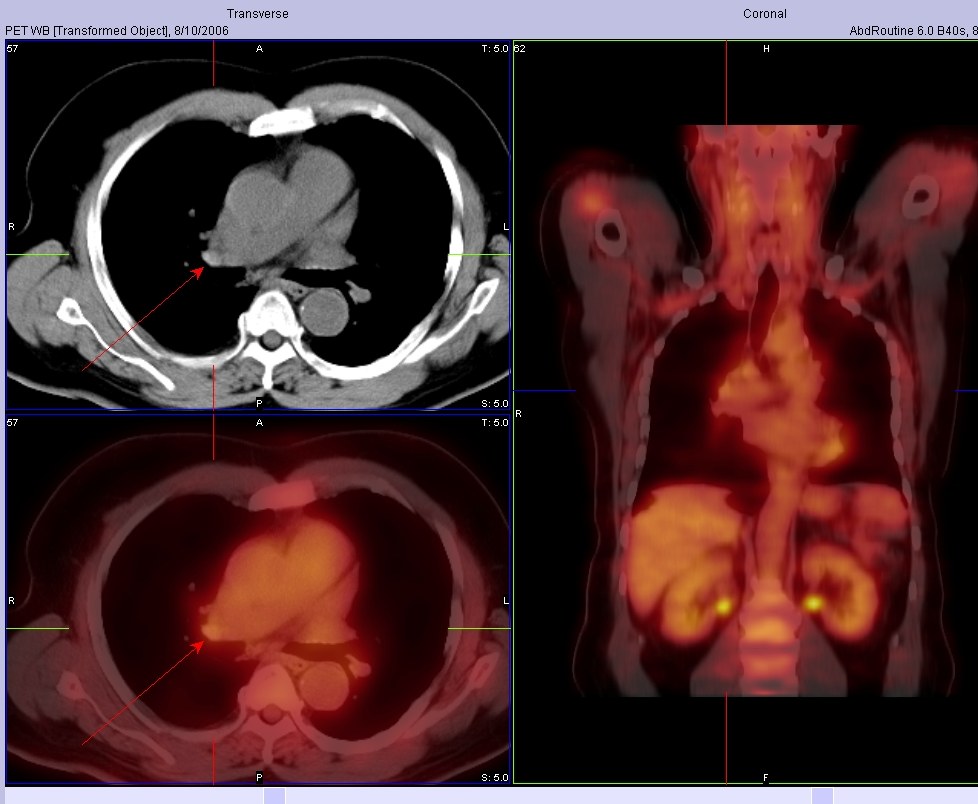
The PET was otherwise negative except for some mild hypermetabolic activity in the right hilar and pericarinal regions corresponding to nonenlarged lymph nodes on CT:
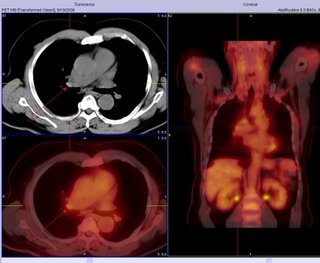
Because of this, he underwent LUL lobectomy. However, an ipsilateral mediastinal node was positive. I do not think they sampled the area of the hilum that lit up (it was contralateral), so in this case the PET did not indicate that he had spread. Also of interest, the margins from resected mass were negative.

The PET was otherwise negative except for some mild hypermetabolic activity in the right hilar and pericarinal regions corresponding to nonenlarged lymph nodes on CT:
Because of this, he underwent LUL lobectomy. However, an ipsilateral mediastinal node was positive. I do not think they sampled the area of the hilum that lit up (it was contralateral), so in this case the PET did not indicate that he had spread. Also of interest, the margins from resected mass were negative.
Wednesday, October 25, 2006
Preop eval for secondary HTN due to severe COPD
Redneck pulmonologist submits this question:
Would you do anything for secondary pulmonary hypertension (estimated PAP of 80-90 mmHG on echo) due to COPD before undergoing renal transplant? Her COPD is 2 to AAT deficiency and stable on AAT replacement. FEV1 of 40% predicted. She has documented nocturnal desat on sleep study without significant sleep apnea. But she is non-compliant with home O2. Daytime sat on RA is OK. She is not a smoker. She is on dialysis and her ESRD is due to pauci-immune vasculitis and has been treated with steroids and Cellcept. Work up for other causes of secondary pulmonary HTN is negative.
Would you do anything for secondary pulmonary hypertension (estimated PAP of 80-90 mmHG on echo) due to COPD before undergoing renal transplant? Her COPD is 2 to AAT deficiency and stable on AAT replacement. FEV1 of 40% predicted. She has documented nocturnal desat on sleep study without significant sleep apnea. But she is non-compliant with home O2. Daytime sat on RA is OK. She is not a smoker. She is on dialysis and her ESRD is due to pauci-immune vasculitis and has been treated with steroids and Cellcept. Work up for other causes of secondary pulmonary HTN is negative.
Wednesday, July 26, 2006
LVRS contra-indication
This question came up recently on this patient's follow-up. This is a relatively young man with HIV/AIDS who has done remarkably well on HAART (he had PCP 8 years ago!). He has the typical bullous emphysema associated with HIV and his previous smoking history. His emphysema is predominantly upper lobe (see below with a nice azygous "lobe"), he is hyperinflated and has air trapping. His FEV1 is still greater than 45% so LVRS is not for him yet anyway.
However, the question came up, is HIV infection an absolute contra-indication to LVRS?

However, the question came up, is HIV infection an absolute contra-indication to LVRS?

Monday, June 05, 2006
Timing of surgeries
This is a 65 y/o man transferred to our hospital for CP. He was found to have an acute coronary syndrome and a lung mass. He underwent a cardiac cath ahich revealed diffuse disease: 20% LM, an occlude LAD with R-L and L-L shunt with a large patent ramus and RCA disease. In addition to his acute care he needs a CABG. He had a stent placed in his RCA, received Plavix and ASA for a month and we stopped it so we could work up his mass.
A bronch confirmed that this is a NSCLCa (squamous cell). His PET scan only lit up on the mass and nowhere else. His PFTs are not great but could tolerate a lobectomy.
How would time the cardiac work up and the planning of surgery for his lung Ca?
Thursday, March 23, 2006
LVRS
Steve G. asks about lung volume reduction requirements. In a patient with heterogeneous emphysema in the upper lobes, what defines poor exercise tolerance? Is an exercise study necessary or can we use the 6 minute walk to evaluate? If so, how many meters would be considered poor?
Subscribe to:
Posts (Atom)