Unfortunately, our computer is not letting me retrieve the PET images on this patient so I'll try and describe it without puppets.
This is a 71 y/o man with long TOB Hx but still good mechanics (FEV1~78%) with a new lung mass. He was found to have a 2.5-cm mass in the RML and had a CT-guided Bx which was + for adenoCa. He then had a PET and came to see us: the mass was obviously hot but he had FDG-avid subcarinal and L hilar nodes and a 1-cm FDG-avid LUL peripheral lesion. I bronch'ed him and sampled his nodes and got lots of giant cells and lymphocytes but no malignancy (from both sites). A LUL BAL was non-Dx.
Would you Bx the LUL separately? And if so how would you approach this (synchronous vs metastatic lesions, etc.)?
Showing posts with label Lung cancer. Show all posts
Showing posts with label Lung cancer. Show all posts
Wednesday, April 04, 2007
Tuesday, February 06, 2007
Alternatives to surgery
Following Jeff's question on therapy for lung Ca in octogenarian (see post below) I just saw a patient in a similar situation. This is an 85 y/o woman with a recent spiro revealing an FEV1 of 600 ml. She was just diagnosed with a 2-cm LUL adenoCa with no adenopathy and no other distant disease on PET. She is still fairly active but stated that even if her lung function improved, she would not want surgery.
With such a low FEV1 and with some risk of further loss of function with radiation, what would you suggest? And following on JJ's question, what are your alternatives for octogenarians (or anybody else) who can't or won't have surgery?
With such a low FEV1 and with some risk of further loss of function with radiation, what would you suggest? And following on JJ's question, what are your alternatives for octogenarians (or anybody else) who can't or won't have surgery?
Tuesday, January 30, 2007
This is an 89 year old previous smoker with a probably stage 1b cancer:
No adenopathy.
She looks younger than her stated age but has emphysema on CXR:

We dont have PFT's but she has good exercise tolerance.
How would you proceed assuming the patient was willing to go with whatever the doctor recommends:
1. surgery (is age alone an absolute contraindication, even if she would otherwise be a surgical candidate)?
2. CT-guided bx (but what would you do with this info? it is obviously a cancer. Would you offer this 89 year old chemo?)
3. Do nothing.
4. Other.
Looking for all opinions - use anonymous or make up a name if you wish, but all comments encouraged.

No adenopathy.
She looks younger than her stated age but has emphysema on CXR:

We dont have PFT's but she has good exercise tolerance.
How would you proceed assuming the patient was willing to go with whatever the doctor recommends:
1. surgery (is age alone an absolute contraindication, even if she would otherwise be a surgical candidate)?
2. CT-guided bx (but what would you do with this info? it is obviously a cancer. Would you offer this 89 year old chemo?)
3. Do nothing.
4. Other.
Looking for all opinions - use anonymous or make up a name if you wish, but all comments encouraged.
Tuesday, November 21, 2006
CXR followup after resection
A curious reader from Maine would like to know:
How frequently and for how long, do you follow xray/CT's after the surgical resection of a stage 2 lung cancer.
How frequently and for how long, do you follow xray/CT's after the surgical resection of a stage 2 lung cancer.
Friday, November 03, 2006
preop stage
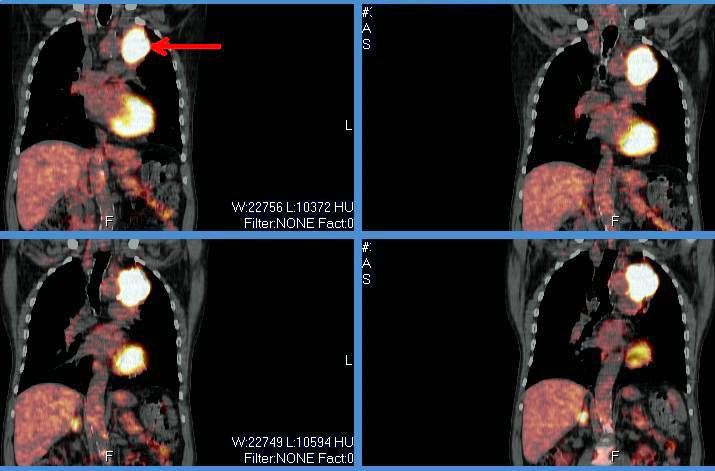
I thought this was an interesting case because it involves role and possible limitations of PET scanning for staging prior to surgical resection. A 69 year old presented with a LUL mass. The bronch brushings revealed non-small cell lung cancer. A PET showed the intense uptake in that mass:
The PET was otherwise negative except for some mild hypermetabolic activity in the right hilar and pericarinal regions corresponding to nonenlarged lymph nodes on CT:
Because of this, he underwent LUL lobectomy. However, an ipsilateral mediastinal node was positive. I do not think they sampled the area of the hilum that lit up (it was contralateral), so in this case the PET did not indicate that he had spread. Also of interest, the margins from resected mass were negative.

The PET was otherwise negative except for some mild hypermetabolic activity in the right hilar and pericarinal regions corresponding to nonenlarged lymph nodes on CT:
Because of this, he underwent LUL lobectomy. However, an ipsilateral mediastinal node was positive. I do not think they sampled the area of the hilum that lit up (it was contralateral), so in this case the PET did not indicate that he had spread. Also of interest, the margins from resected mass were negative.
Wednesday, November 01, 2006
Follow-up to Abnormal CxR
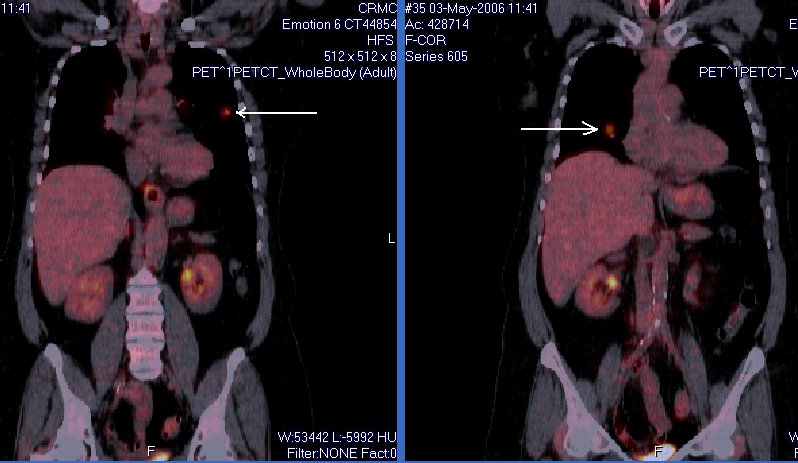
This is my VIP patient who got to see us and Hem-Onc at the same time and had a Squam on a CT-guided Bx.
She then had a PET scan which lit up on the mass and on a small (<1 cm) ipsilateral hilar lymph node.
She underwent a med which showed only reactive adenopathy. She had a lobectomy 2 days ago with a T2 squam with negative margins and negative nodes.
At your institution, would you offer adjuvant chemo, xRt, both or neither at this point?
She then had a PET scan which lit up on the mass and on a small (<1 cm) ipsilateral hilar lymph node.
She underwent a med which showed only reactive adenopathy. She had a lobectomy 2 days ago with a T2 squam with negative margins and negative nodes.
At your institution, would you offer adjuvant chemo, xRt, both or neither at this point?
Monday, October 30, 2006
The Philosophy of Disclosure
From AK:
I'm sure most of us have seen some close variation on this clinical theme: a smoker has a suspicious lung mass with evidence of metastasis elsewhere, and you're consulted to help get tissue. The patient hasn't seen the scans, doesn't know the overwhelming odds that they have metastatic lung cancer. As a consultant, how much should you tell the patient before you have path results? If they ask about the possibility of surgical resection, is it right to put off an answer you know is highly likely to be correct?
I'm sure most of us have seen some close variation on this clinical theme: a smoker has a suspicious lung mass with evidence of metastasis elsewhere, and you're consulted to help get tissue. The patient hasn't seen the scans, doesn't know the overwhelming odds that they have metastatic lung cancer. As a consultant, how much should you tell the patient before you have path results? If they ask about the possibility of surgical resection, is it right to put off an answer you know is highly likely to be correct?
Thursday, October 26, 2006
Lung cancer screening
The International Early Lung Cancer Action Program Investigators published the results from CT screening >30,000 patients with chest CTs in today's NEJM.
They found a shift towards picking up more early stage disease.
Have you had a chance to see the study? How do you think this will affect our practice?
They found a shift towards picking up more early stage disease.
Have you had a chance to see the study? How do you think this will affect our practice?
Tuesday, October 17, 2006
Abnormal CxR
I usually don't like those boards-type question that ask "what would you do next?" and only let you choose one option since we often do more than one thing in real life.
Having said that, I am curious as to what you would do next in this case. This is kind of a VIP patient so she was referred to a couple different specialists at the same time.
She is in her early 70s, quit smoking in 1972, near normal PFTs (FEV1~70%, normal DLCO) and has an abnormal CxR. It started as an URI and then she developed a "deeper" cough with purulent sputum production and some pleuritic CP.
The abnormal CxR (and some CT cuts) are shown below.
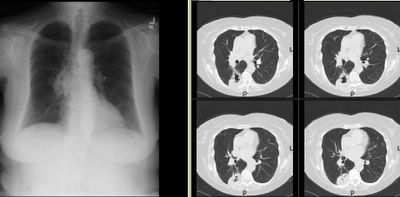
She had no adenopathy on the CT.
What would be your first step?
Having said that, I am curious as to what you would do next in this case. This is kind of a VIP patient so she was referred to a couple different specialists at the same time.
She is in her early 70s, quit smoking in 1972, near normal PFTs (FEV1~70%, normal DLCO) and has an abnormal CxR. It started as an URI and then she developed a "deeper" cough with purulent sputum production and some pleuritic CP.
The abnormal CxR (and some CT cuts) are shown below.

She had no adenopathy on the CT.
What would be your first step?
Thursday, September 07, 2006
Advice on further workup for this lung cancer.
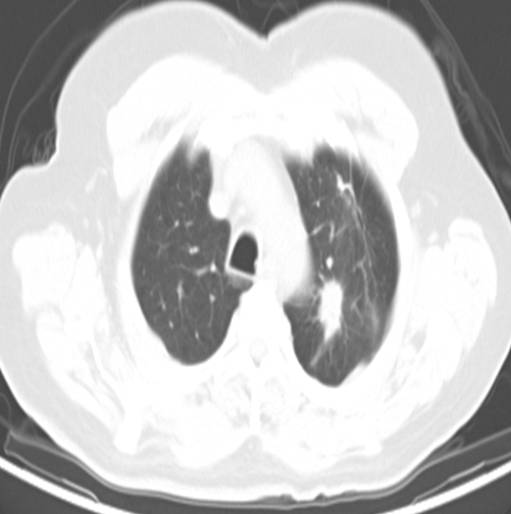
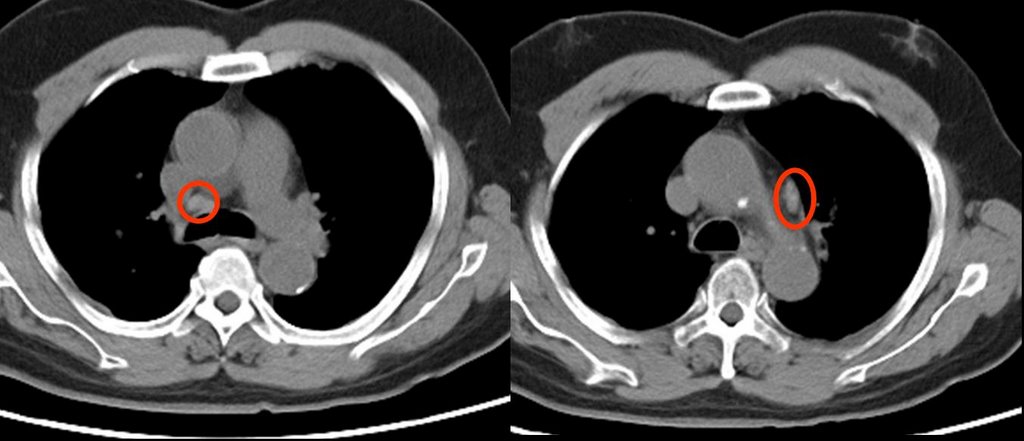
59 year old ex-smoker with FEV1 1.17 liters (47% predicted) who has a left upper lobe lesion:
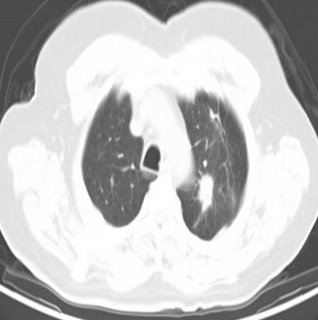
He also has some enlarged nodes (red circles):
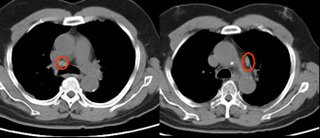
The PET showed intense uptake of the LUL lesion and "mild hypermetabolic activity in the right hilar and pericarinal regions corresponding to nonenlarged lymph nodes on CT. This is of uncertain clinical significance. No other foci of abnormal hypermetabolic activity are identified.":
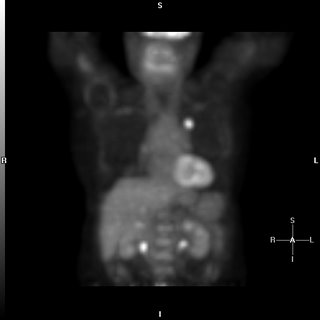
However, because of the enlarged nodes and the equivocal uptake on PET , I elected to sample them anyway;
The results showed no malignancy from the fine needle aspirate (but there were lymphocytes indicating that the node was sampled.
Not surprisingly, biopsy of the peripheral lesion in the LUL lesion was indeed cancer - adenocarcinoma.
Would you call this cancer a stage I (tumor was 2.4 x 1.4 cm) and proceed to surgery?
He also has some enlarged nodes (red circles):
The PET showed intense uptake of the LUL lesion and "mild hypermetabolic activity in the right hilar and pericarinal regions corresponding to nonenlarged lymph nodes on CT. This is of uncertain clinical significance. No other foci of abnormal hypermetabolic activity are identified.":

However, because of the enlarged nodes and the equivocal uptake on PET , I elected to sample them anyway;
The results showed no malignancy from the fine needle aspirate (but there were lymphocytes indicating that the node was sampled.
Not surprisingly, biopsy of the peripheral lesion in the LUL lesion was indeed cancer - adenocarcinoma.
Would you call this cancer a stage I (tumor was 2.4 x 1.4 cm) and proceed to surgery?
Wednesday, August 30, 2006
Diagnosis and staging of lung cancer
Anonymous asks, If a patient, on chest CT, has a mass invading the hilum and mediastinum and there is also a pleural effusion, would you be able to simply do a thoracentesis for cytology and forego the bronch?
My take is that a bronchoscopy would not be neccessary, as a positive effusion will both diagnose and stage it as a T4. What do you think?
My take is that a bronchoscopy would not be neccessary, as a positive effusion will both diagnose and stage it as a T4. What do you think?
Tuesday, August 15, 2006
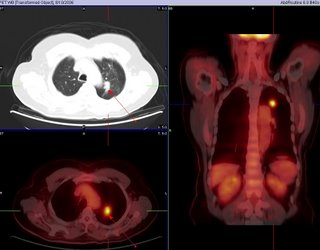
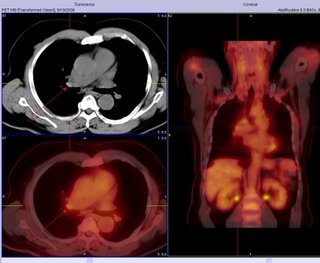
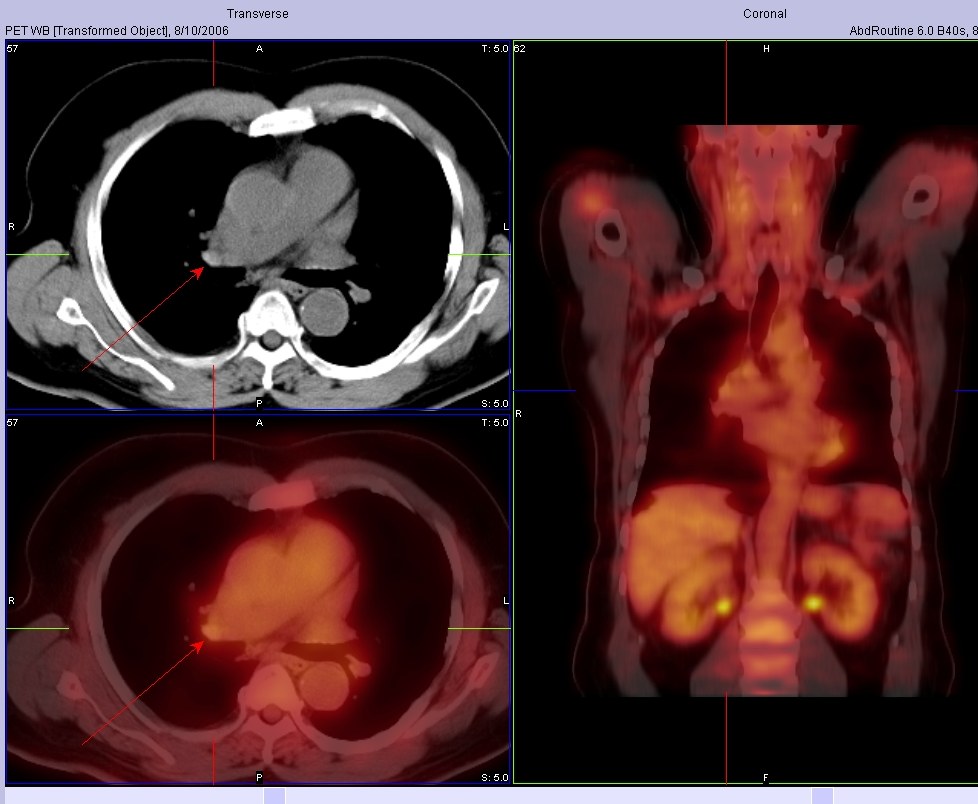
PET and staging
I saw this patient in follow-up today.
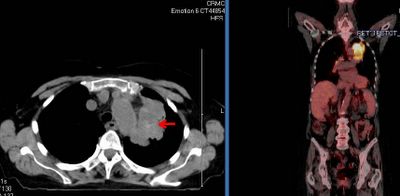
This is an 82 y/o woman with no smoking history but decades of second-hand smoke (her husband died of lung dz). She had a dry cough and a CT scan was done. She has the large LUL mass seen on the CT cut (on an outside CT with contrast, the mass seems to invade the PA). I did a bronch and the mass is a non-small cell Ca. Unfortunately, the hilar TBNA were non-diagnostic. Her PET scan shows marked uptake by the mas, ipsi- and contralateral hilar nodes and pre-tracheal nodes.
With the PA involvement (on CT) and the PET results would you be satisfied in calling it a IIIB or would you do a mediastinoscopy to confirm either/both with tissue?
This is an 82 y/o woman with no smoking history but decades of second-hand smoke (her husband died of lung dz). She had a dry cough and a CT scan was done. She has the large LUL mass seen on the CT cut (on an outside CT with contrast, the mass seems to invade the PA). I did a bronch and the mass is a non-small cell Ca. Unfortunately, the hilar TBNA were non-diagnostic. Her PET scan shows marked uptake by the mas, ipsi- and contralateral hilar nodes and pre-tracheal nodes.
With the PA involvement (on CT) and the PET results would you be satisfied in calling it a IIIB or would you do a mediastinoscopy to confirm either/both with tissue?

Wednesday, August 09, 2006
Proceed or watch? Is it CA?
Here is a case submitted to us:
8/1/06 49 YO Caucasion male, married with minor children, comfortably employed professional, USAF Gulf War Veteran, 2-3 PPD smoker X30 years, ETOH dependent (averages 6-10 beers daily)presents with R clavicular pain after home remodeling project. Well developed, well nourished, muscular, athletic body type. VS WNL. Non remarkable EKG. Clavicle XR demonstrates shoulder separation with incidental 1.75cm diameter spiculated nodule mid upper right lobe lung, mild emphysematous changes. CT confirms nodule. PET eyes to knees results no demonstrative uptakes. CBC, Metabolic panels normal. CEA and CA125 WNL. PFTs near normal, demonstrates ability to tolerate surgery.
Family HX: Maternal died d/t +NSCL CA with brain, liver mets. Paternal +adenocarcinoma colon, in remission post colectomy and chemo. No other significant family HX or disease.
Smoking Cessation in process with nicotine patch use. ETOH use diminishing. Pt. wants no invasive surgery or BX unless absolutely indicated. Lesion is not near bronch, no bronchoscopy in plan. What next?
8/1/06 49 YO Caucasion male, married with minor children, comfortably employed professional, USAF Gulf War Veteran, 2-3 PPD smoker X30 years, ETOH dependent (averages 6-10 beers daily)presents with R clavicular pain after home remodeling project. Well developed, well nourished, muscular, athletic body type. VS WNL. Non remarkable EKG. Clavicle XR demonstrates shoulder separation with incidental 1.75cm diameter spiculated nodule mid upper right lobe lung, mild emphysematous changes. CT confirms nodule. PET eyes to knees results no demonstrative uptakes. CBC, Metabolic panels normal. CEA and CA125 WNL. PFTs near normal, demonstrates ability to tolerate surgery.
Family HX: Maternal died d/t +NSCL CA with brain, liver mets. Paternal +adenocarcinoma colon, in remission post colectomy and chemo. No other significant family HX or disease.
Smoking Cessation in process with nicotine patch use. ETOH use diminishing. Pt. wants no invasive surgery or BX unless absolutely indicated. Lesion is not near bronch, no bronchoscopy in plan. What next?
Thursday, August 03, 2006
Halleliujah
From Arenberg:
"In celebration of the fact that the IT people in the Department of Radiology at the University of of Michigan have recognozed that their department exists to provide films for other doctors to look at, and have finally made it into the 21st centry by providing consistent, relaible online access to films for the unwashed masses (read: non-radiologists)...I hereby submit this film of an unfortunate man with a history of cancer."

"In celebration of the fact that the IT people in the Department of Radiology at the University of of Michigan have recognozed that their department exists to provide films for other doctors to look at, and have finally made it into the 21st centry by providing consistent, relaible online access to films for the unwashed masses (read: non-radiologists)...I hereby submit this film of an unfortunate man with a history of cancer."

Thursday, July 20, 2006
Radiation and lung cancer
I think it is my week to pick on radiation Tx... I already posted on the time delay notion (BTW, check out the PPT on that listed on the comments section).
What is your impression/practice on the use of xRt and lung cancer?
It certainly has an excellent role in symptom palliation, particularly with painful bony mets and other solitary mets presentations. It does decrease local recurrence (though it has less of an impact on survival) in locally advanced disease but it seems to me that it is automatically lumped with chemo as if you must have one with the other.
As a single modality (“curative xRt”) kind of falls short:
In a review of ten studies that utilized megavoltage irradiation to doses of >55 gray (Gy) in conventional fractionation for patients with medically inoperable Stage I lung carcinoma, only approximately 15% of patients were long term survivors (vs surgery and multimodality Tx). Cancer 1998 Feb 1;82(3):433-8
Similarly, five-year survival was only 19 percent in a series of "medically inoperable" patients with stage II disease. Radiat Oncol Invest 1996; 4:165
And the data on post-op xRt is not as good as post-op chemo:
In a French trial of post-op xRt vs. observation only, five-year overall survival was 43% for the control group and 30% for the radiotherapy group (P = 0.002). Cancer 1999 Jul 15;86(2):265-73
The older Lung Cancer Study Group from 86 showed no evidence that radiotherapy improved survival, and although recurrence rates appeared to be somewhat reduced among patients assigned to radiotherapy, these decreases were not statistically significant. N Engl J Med 1986 Nov 27;315(22):1377-81
In the IALT trial, which focused on post-op therapy and showed a benefit for chemo,
only 70.4 percent of those assigned to receive adjuvant thoracic radiotherapy in the chemotherapy group actually received xRt and the control group had actually a higher rate of xRt. N Engl J Med 2004 Jan 22;350(4):351-60
The PORT meta-analysis even showed a significant adverse effect of postoperative radiotherapy on survival (hazard ratio 1.21 [95% CI 1.08-1.34]). Lancet. 1998 Jul 25;352(9124):257-63
Even in stage III dz, whether they have N2 dz or a T4 things are not that clear:
Patients with non-small cell lung cancer who had inoperable, nonmetastatic disease gained no clinically meaningful survival advantage with immediate thoracic irradiation, even when modern megavoltage radiation therapy techniques and equipment was used in Ann Intern Med 1990 Jul 1;113(1):33-8. And in minimally symptomatic patients with locally advanced non-small cell lung cancer, “no persuasive evidence was found to indicate that giving immediate palliative thoracic radiotherapy improves symptom control, quality of life, or survival when compared with delaying until symptoms require treatment”. BMJ 2002 Aug 31;325(7362):465
What do you think?
What is your impression/practice on the use of xRt and lung cancer?
It certainly has an excellent role in symptom palliation, particularly with painful bony mets and other solitary mets presentations. It does decrease local recurrence (though it has less of an impact on survival) in locally advanced disease but it seems to me that it is automatically lumped with chemo as if you must have one with the other.
As a single modality (“curative xRt”) kind of falls short:
In a review of ten studies that utilized megavoltage irradiation to doses of >55 gray (Gy) in conventional fractionation for patients with medically inoperable Stage I lung carcinoma, only approximately 15% of patients were long term survivors (vs surgery and multimodality Tx). Cancer 1998 Feb 1;82(3):433-8
Similarly, five-year survival was only 19 percent in a series of "medically inoperable" patients with stage II disease. Radiat Oncol Invest 1996; 4:165
And the data on post-op xRt is not as good as post-op chemo:
In a French trial of post-op xRt vs. observation only, five-year overall survival was 43% for the control group and 30% for the radiotherapy group (P = 0.002). Cancer 1999 Jul 15;86(2):265-73
The older Lung Cancer Study Group from 86 showed no evidence that radiotherapy improved survival, and although recurrence rates appeared to be somewhat reduced among patients assigned to radiotherapy, these decreases were not statistically significant. N Engl J Med 1986 Nov 27;315(22):1377-81
In the IALT trial, which focused on post-op therapy and showed a benefit for chemo,
only 70.4 percent of those assigned to receive adjuvant thoracic radiotherapy in the chemotherapy group actually received xRt and the control group had actually a higher rate of xRt. N Engl J Med 2004 Jan 22;350(4):351-60
The PORT meta-analysis even showed a significant adverse effect of postoperative radiotherapy on survival (hazard ratio 1.21 [95% CI 1.08-1.34]). Lancet. 1998 Jul 25;352(9124):257-63
Even in stage III dz, whether they have N2 dz or a T4 things are not that clear:
Patients with non-small cell lung cancer who had inoperable, nonmetastatic disease gained no clinically meaningful survival advantage with immediate thoracic irradiation, even when modern megavoltage radiation therapy techniques and equipment was used in Ann Intern Med 1990 Jul 1;113(1):33-8. And in minimally symptomatic patients with locally advanced non-small cell lung cancer, “no persuasive evidence was found to indicate that giving immediate palliative thoracic radiotherapy improves symptom control, quality of life, or survival when compared with delaying until symptoms require treatment”. BMJ 2002 Aug 31;325(7362):465
What do you think?
Monday, June 12, 2006
Stenting and lung cancer
Just curious what you all think of the role of stenting in advanced lung cancer. This obviously would not effect such hard endpoins as survival, but it seems to alleviate dyspnea and might mpact on quality of life. Unfortunately I do not think there is much data out there to support this, but this does not necessarily mean that these endpoints are not impacted. Until there is data, what are you all doing with advanced lung ca with regards to interventional bronchoscopy?
Monday, June 05, 2006
Timing of surgeries
This is a 65 y/o man transferred to our hospital for CP. He was found to have an acute coronary syndrome and a lung mass. He underwent a cardiac cath ahich revealed diffuse disease: 20% LM, an occlude LAD with R-L and L-L shunt with a large patent ramus and RCA disease. In addition to his acute care he needs a CABG. He had a stent placed in his RCA, received Plavix and ASA for a month and we stopped it so we could work up his mass.
A bronch confirmed that this is a NSCLCa (squamous cell). His PET scan only lit up on the mass and nowhere else. His PFTs are not great but could tolerate a lobectomy.
How would time the cardiac work up and the planning of surgery for his lung Ca?
Thursday, June 01, 2006
Follow-up to lung nodules
This is the woman with B/L pulmonary nodules. I was also concerned about these non-calcified nodules so she had a PET scan and we performed a bronch. Both nodules lit up on PET and she had some faint, low-SUV uptake in the mediastinal nodes. The TBBx of the R lesion were + for a non-small-cell lung Ca.
She has good PFTs.
What would you do next?
Thursday, May 18, 2006
Lung Ca and estrogen
I had posted below on this complex case of possible HR+ lung Ca and then realized the post was too long and might prevent people from reading all the way to the end so I reposted just the questions:
Lung Ca (particularly adenos) can be receptor positice (I have seen a few references of over 25% positivity). Have you encountered a lot of these ER/PR+ lung Cas and does it have an impact on Tx?
Have you seen many endobronchial mets without parenchymal mets from other sites such as breast?
Lung Ca (particularly adenos) can be receptor positice (I have seen a few references of over 25% positivity). Have you encountered a lot of these ER/PR+ lung Cas and does it have an impact on Tx?
Have you seen many endobronchial mets without parenchymal mets from other sites such as breast?
Tuesday, May 16, 2006
Remote lung Ca and hormone receptors
I had posted this case on two previous posts. This is a 55 y/o remote smoker with a persistent cough who had an abnormal endoBBx (squamous cell Ca) despite a normal CT scan of the chest and a negative PET scan. She had had breast Ca some five yeras ago with mastectomy, chemo/xRt and had some myocardial damage due to the adriamycin.
Many good suggestions were made to the role of inflammation in false-positive biopsies. I sent her to the chair of CT surgery at a nearby large university hospital and he was equally puzzled. While we were debating what to do, she developed new CHF, had a cath, PTCA, PM placed and and AICD. She has ischemic cardiomyopathy and was quite unstable to consider surgery right then and there. She was medically treated for her heart disease, stabilized and reassessed. Unfortunatelly, despite a negative PET three months before, on a repeat CT then PET she now had adenopathy and two small PET+ spinal mets... She was sent to oncologyand though the endoBBx looked like a squam it was poorly differentiated.
The oncologist requested staining for estrogen and progesterone receptos because of the Hx of breats Ca and those were positive.
A couple interesting questions came up.
Lung Ca (particularly adenos) can be receptor positice (I have seen a few references of over 25% positivity). With the receptor positivity would you automatically assume this is a breast Ca? Have you encountered a lot of these ER/PR+ lung Cas and does it have an impact on Tx?
If we regard that as a true late met of breast Ca, have you seen many endobronchial mets as in this case?
Many good suggestions were made to the role of inflammation in false-positive biopsies. I sent her to the chair of CT surgery at a nearby large university hospital and he was equally puzzled. While we were debating what to do, she developed new CHF, had a cath, PTCA, PM placed and and AICD. She has ischemic cardiomyopathy and was quite unstable to consider surgery right then and there. She was medically treated for her heart disease, stabilized and reassessed. Unfortunatelly, despite a negative PET three months before, on a repeat CT then PET she now had adenopathy and two small PET+ spinal mets... She was sent to oncologyand though the endoBBx looked like a squam it was poorly differentiated.
The oncologist requested staining for estrogen and progesterone receptos because of the Hx of breats Ca and those were positive.
A couple interesting questions came up.
Lung Ca (particularly adenos) can be receptor positice (I have seen a few references of over 25% positivity). With the receptor positivity would you automatically assume this is a breast Ca? Have you encountered a lot of these ER/PR+ lung Cas and does it have an impact on Tx?
If we regard that as a true late met of breast Ca, have you seen many endobronchial mets as in this case?
Subscribe to:
Posts (Atom)