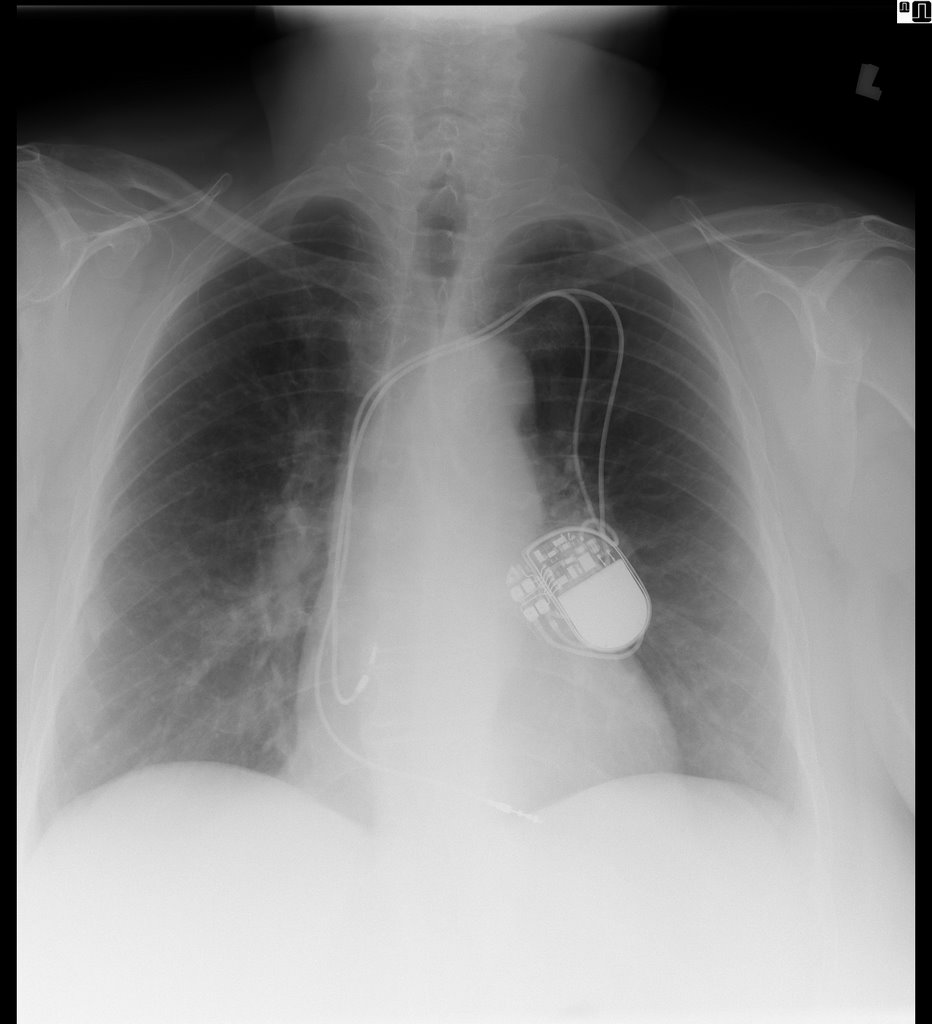
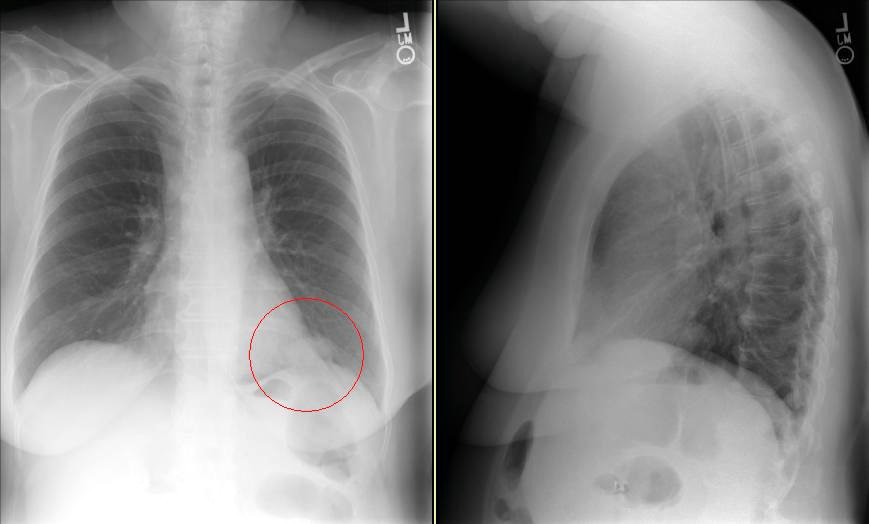
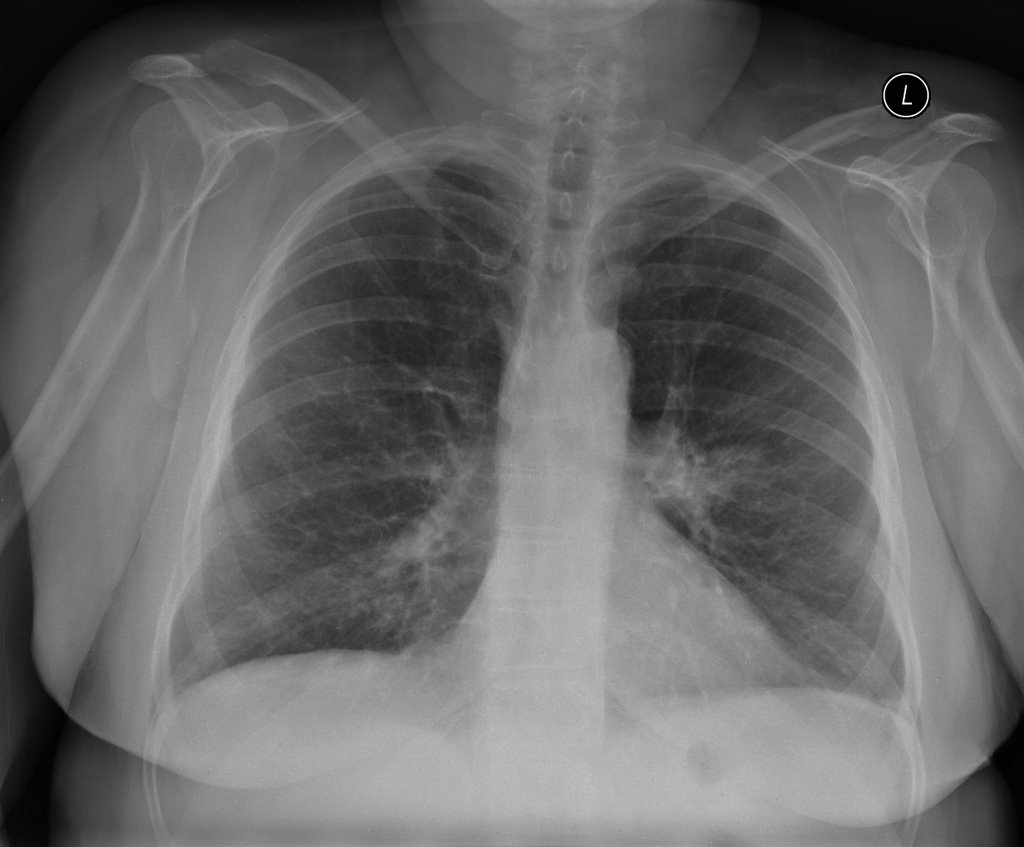
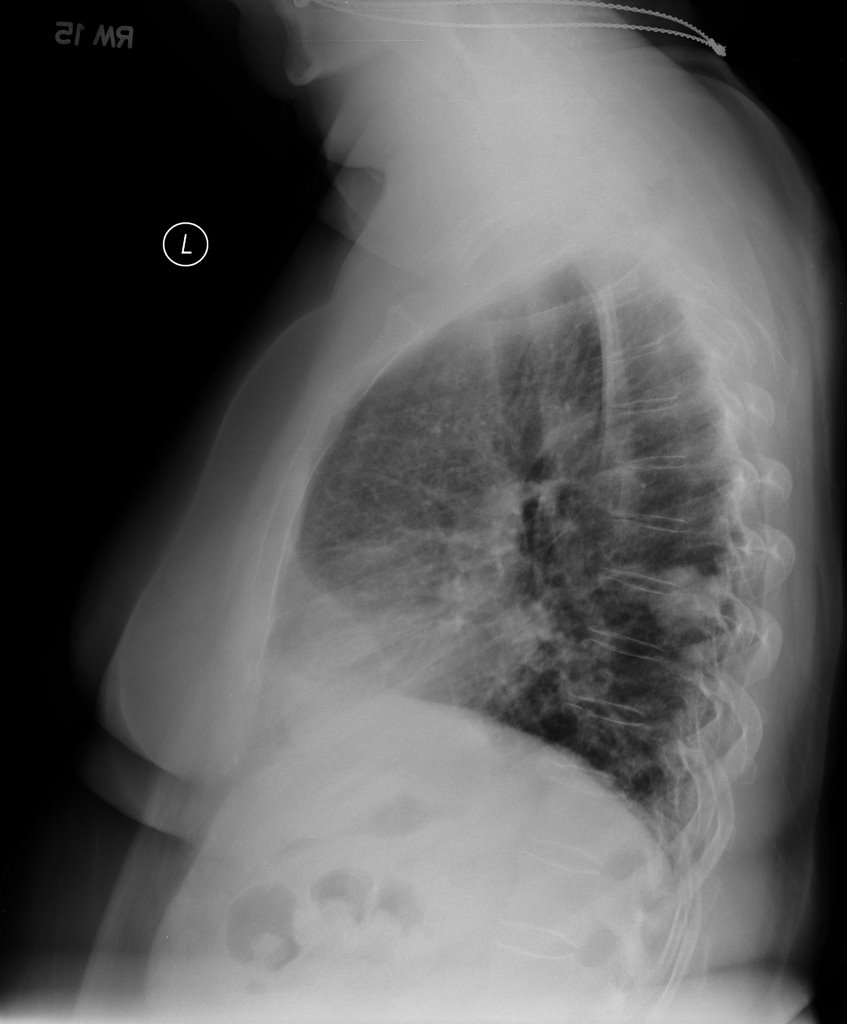
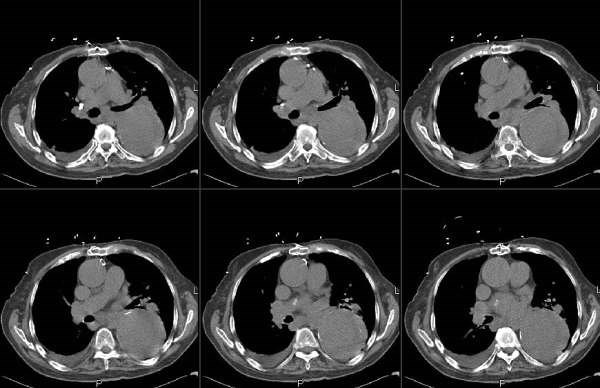
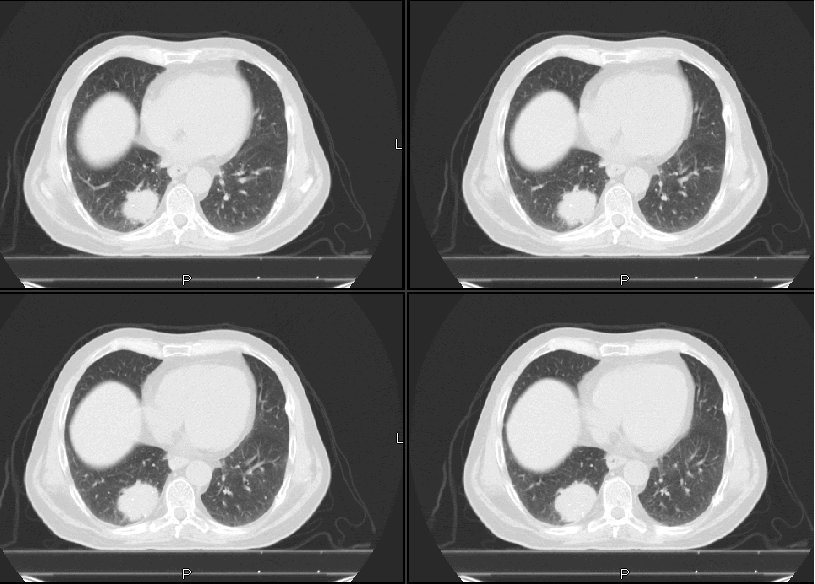
67-year-old Caucasian female who was a previous RN, presents because prior to getting her vascular surgery, she was having a double aortofemoral bypass for claudication. Had a chest x-ray done showed an abnormal opacity on the left lower lobe. She says that she has had worsening shortness of breath for one and half years and has
really had any cough. Denies any fever, chills, rigors, chest pain, or weight loss. Denies any hemoptysis. Denies any previous infections. Denies any headache, nausea, vomiting, or diarrhea.
AST MEDICAL HISTORY: Peripheral vascular disease, hypertension, hyperlipidemia, previous history of smoking.
MEDICATIONS: Atenolol, Protonix, Procardia, hydrochlorothiazide, Lipitor, TriCor, aspirin, multivitamins, and Tylenol 3.
SOCIAL HISTORY: 50-pack-year smoking history, stopped 2 years ago. No ETOH or drug.



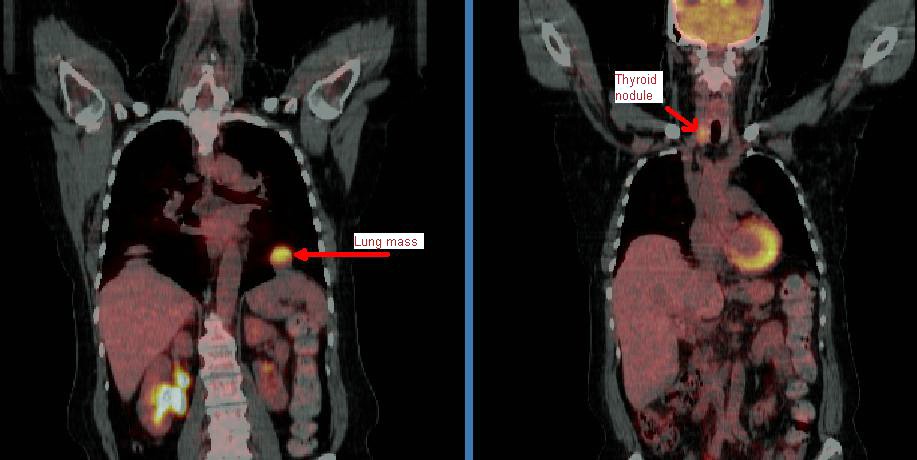
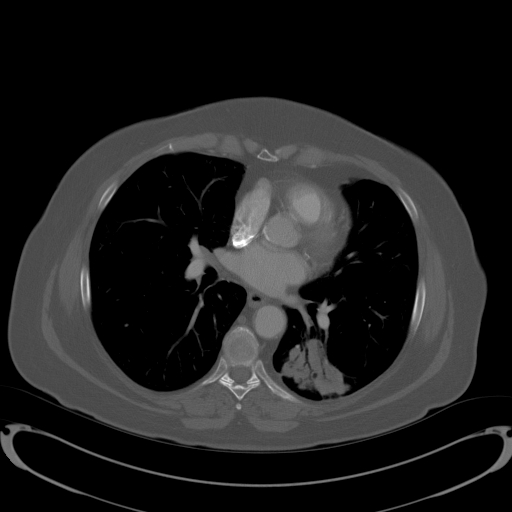
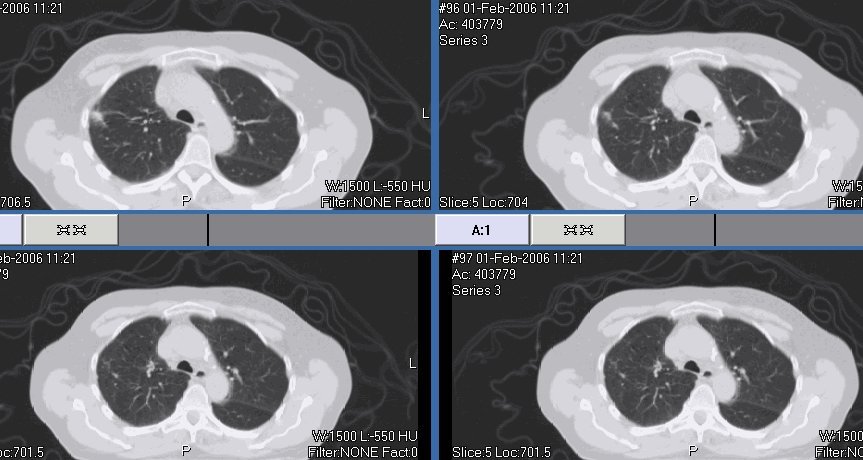
No mediastinal or hilar adenopathy.
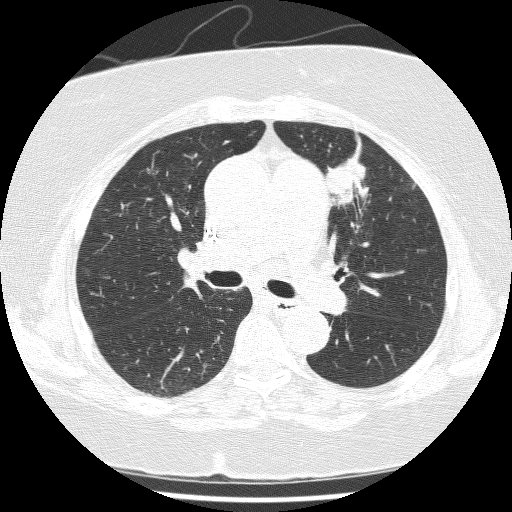
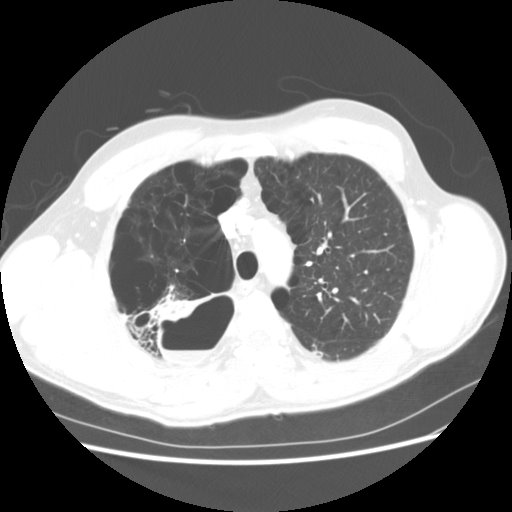
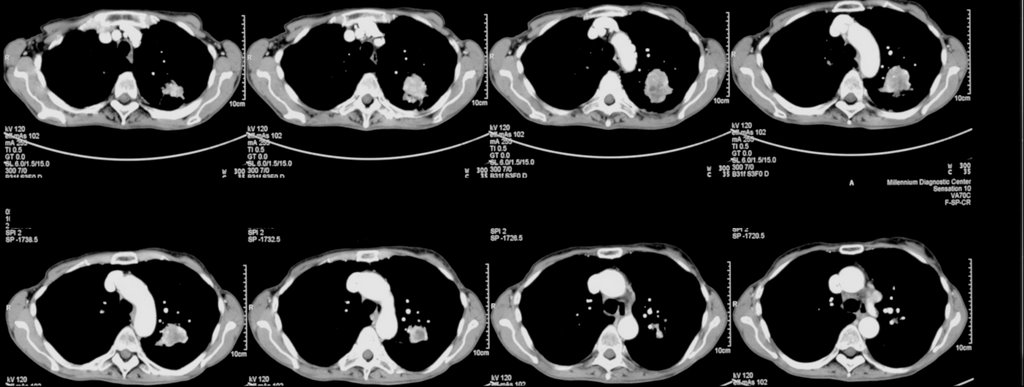
Repeat CT 1 month later showed no change in size.
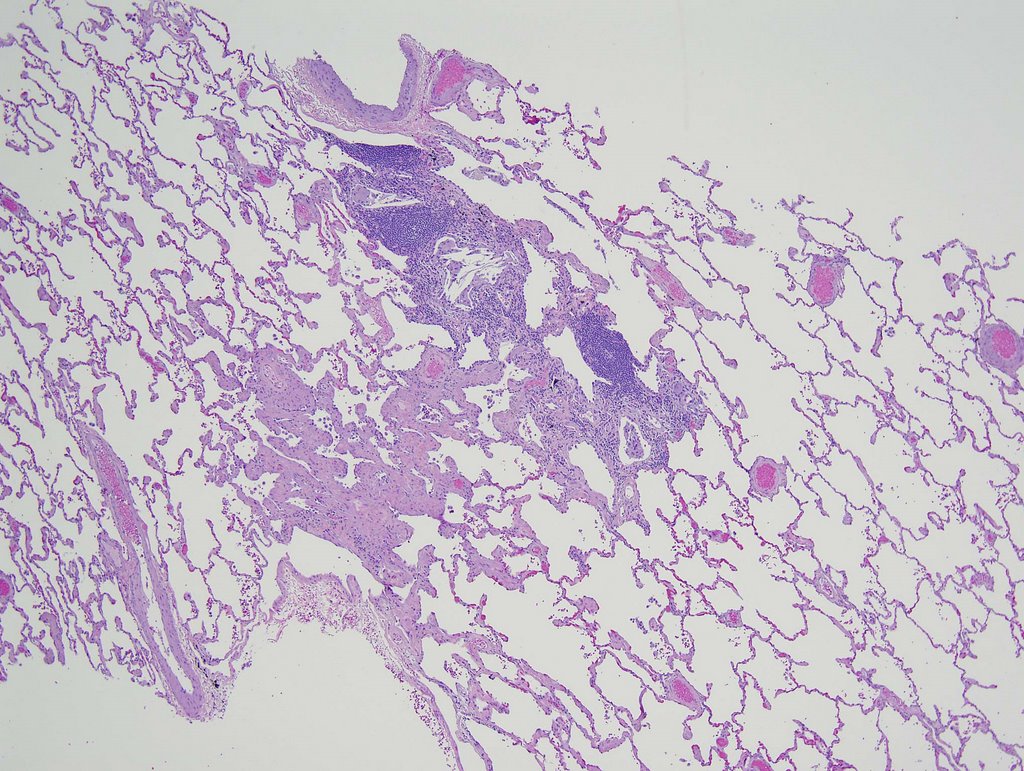
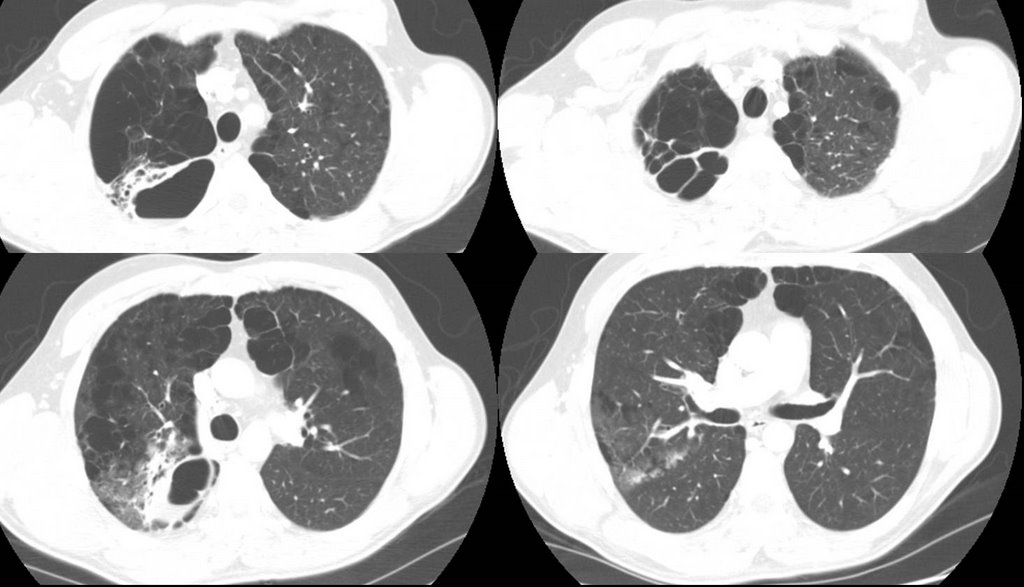
Patient was bronched with non-diagnostic tissue.
Cytology brush from left lower lobe was negative for malignant cells.
Micro on BAL: 30000 CFU per ml alpha-hemolytic Streptococcus, 8000 CFU Neisseria; 9000 CFU Micrococcus; 5000 CFU Streptococcus, non-hemolytic.
What would be your next step (or any other questions you have)?



















{kind=link}
{kind=link}