Friday, December 30, 2005
Happy New Year!
Happy new year from the editors of Pulmonary Roundtable. Please come back and visit us again in 2006.
Thursday, December 29, 2005
Another 80 year old with a lung lesion.
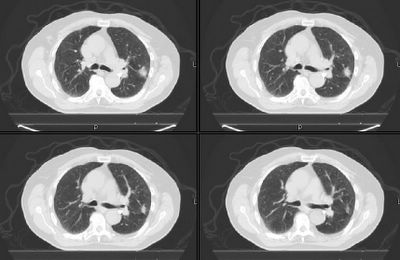
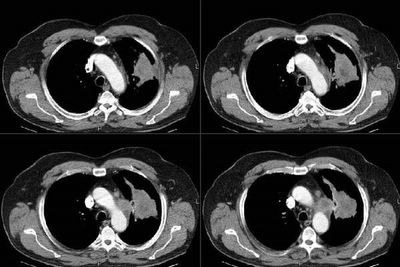
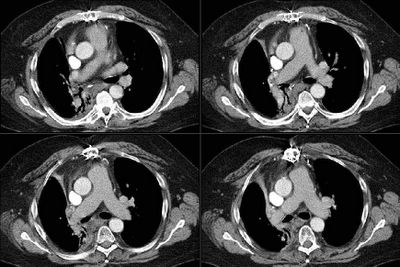
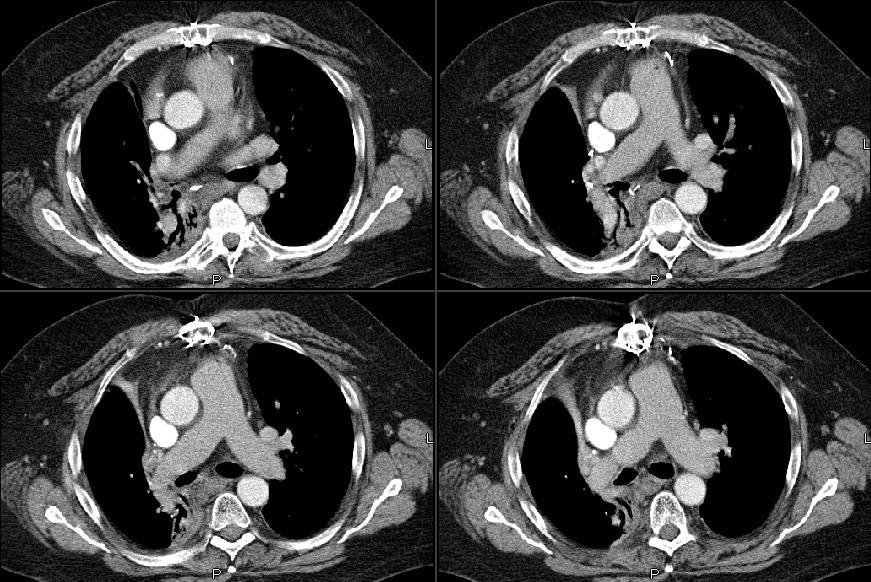
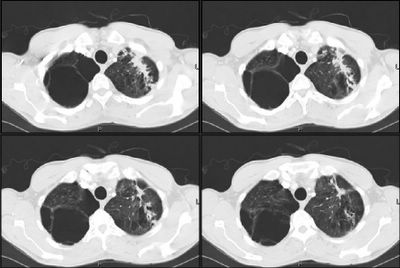
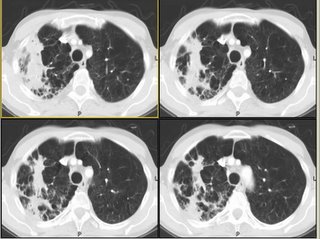
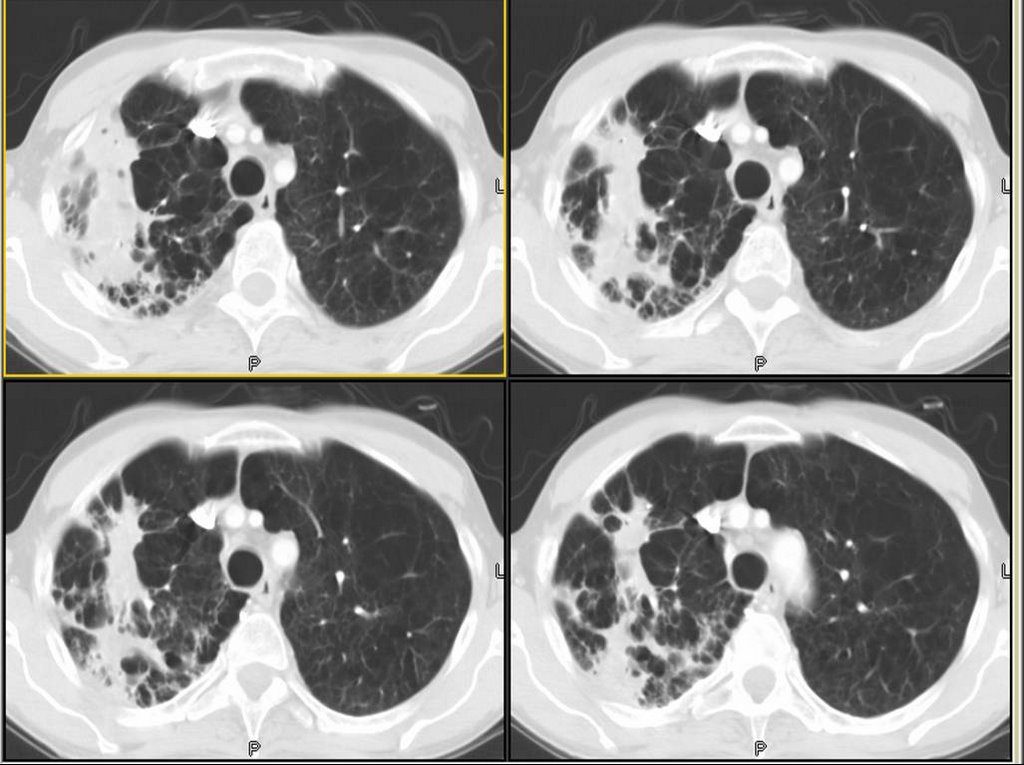
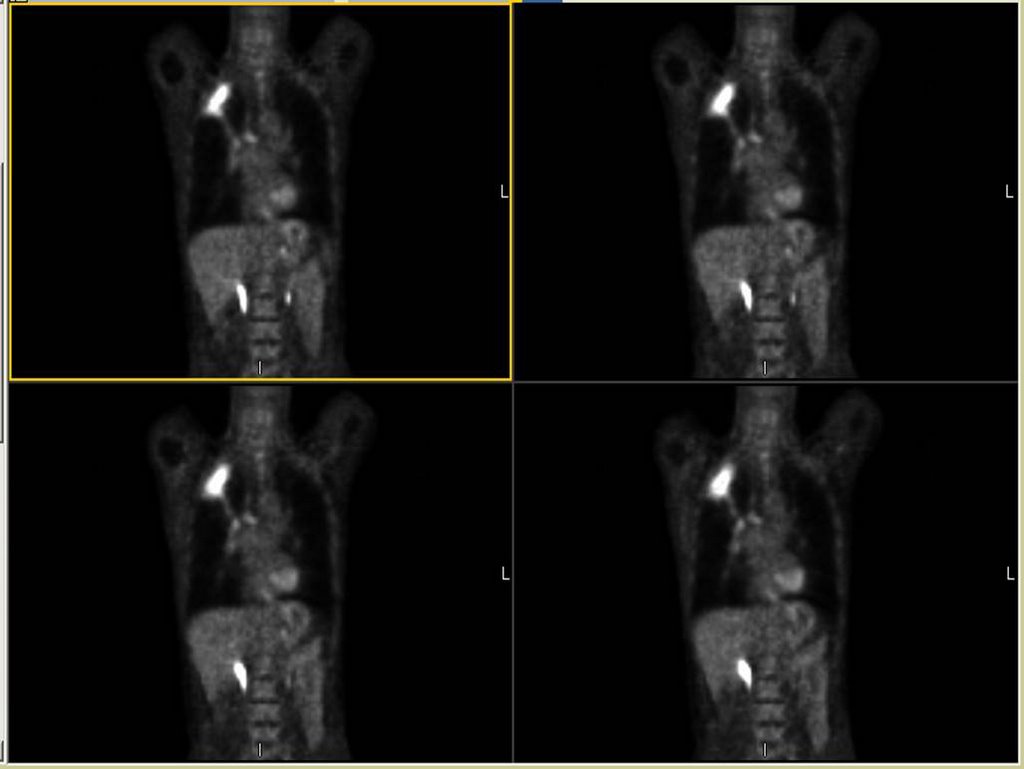
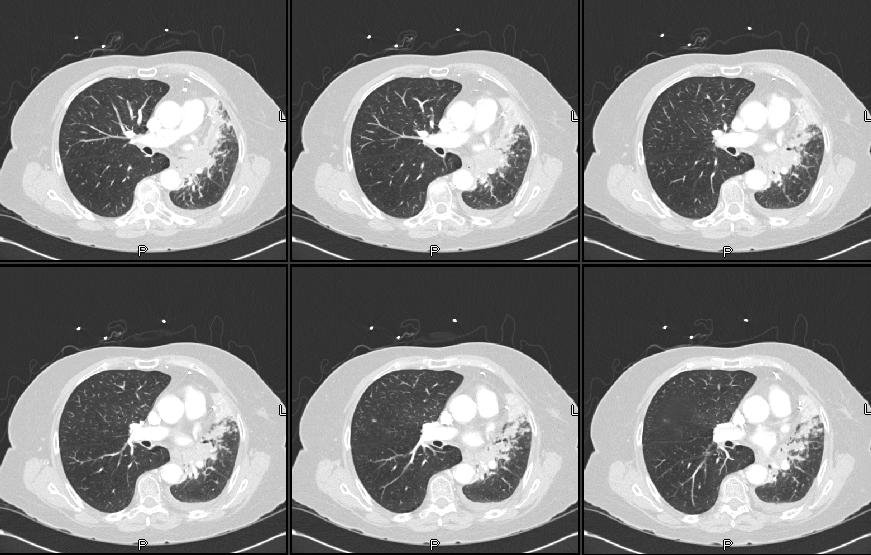
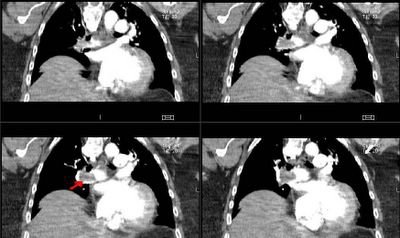
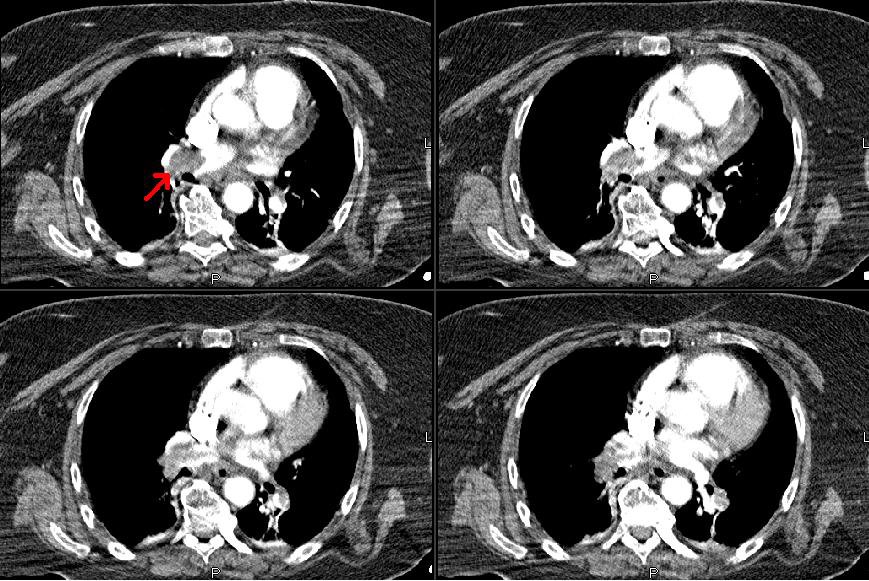
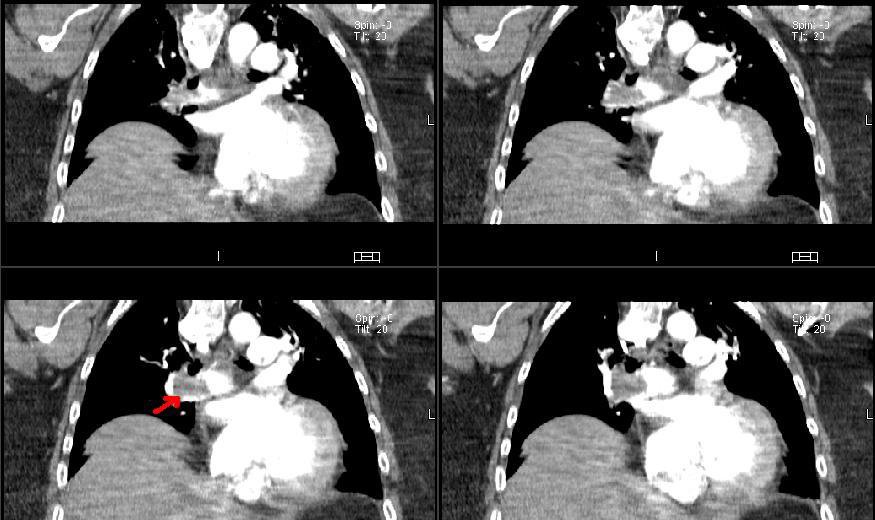
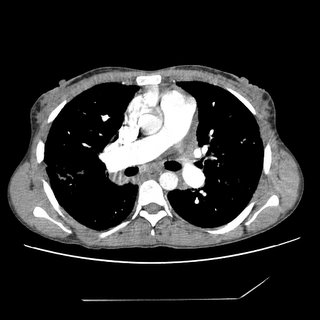
Remember this post about the 80-ish year old with a solitary lesion and whether his age should preclude w/u for possible resection? Well, what would you do with this 82 year old with a hilar (i.e. unresectable) mass that is (as of yet) without diagnosis (i.e. how aggressive would you be with the work-up)?
Here's his CT:

Here's his CT:

Wednesday, December 28, 2005
Abnormal CT scan - part II
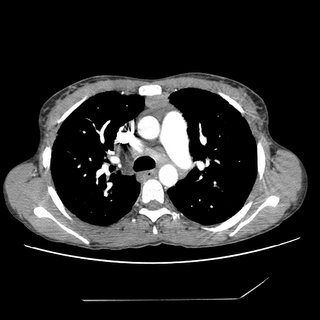
This is the 83 y/o man with the abnormal peripheral lesion. The first post generated an interesting discussion on how old is too old to receive treatment. Since then he has had a PET-CT and a bronch. The lesion looks stable (though only 2 weeks had elapsed) on the CT portion of the PET and there was no abnormal uptake. Hi bronch revealed more airway inflammation on the left bronchial tree than I expected, some Hemophilus but no malignant cells. How would follow him and what would you do next?
Tuesday, December 27, 2005
Patients with treated lung cancer
We see a large number of cases of lung cancer since TN has a rate of TOB use greater than the national average. The American Society of Clinical Oncology does not recommed serial imaging studies for f/up of patients with lung cancer treated with curative intent (lower stages) and there is not very good data on that. How do you usually follow them up?
Wednesday, December 21, 2005
G20210A
Quick question. I have seen this 60 y/o woman in the hospital with B/L pulmonary emboli and DVTs. She has COPD (moderate), OSA and obesity. She was D/C'ed on coumadin and actually received a little over 6 months b/c she underwent a total knee replacement 6 months after the PE. She is now off coumadin, her levels of proteins C&S and ATIII are normal but she is heterozygous for the prothrombin gene mutation at AA 20210. This is a first episode of VTE but she had a lot of clot in her CT with a single genetic defect (no factor V Leiden). Would you recommend indefinite anticoagulation?
Follow-up to pulmonary infiltrates
This is the 68 y/o man post-ABVD for Hodgkin's described below. He had a bronch this week: bal was cloudy but not purulent or bloody; smears and stains were negative for any organisms, no increase in Eos, no giant cells. TBBx revealed diffuse alveolar damage with edema, an inflammatory infiltrate, no organisms, no lymphoma and changes were consistent with Bleo toxicity. He is still on ABTx and quite hypoxic so we are planning on pulsing him with Solu-medrol.
Tuesday, December 20, 2005
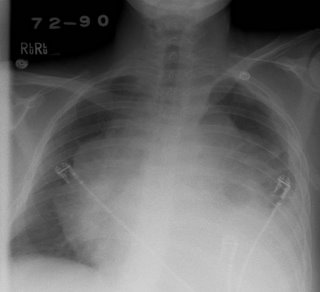
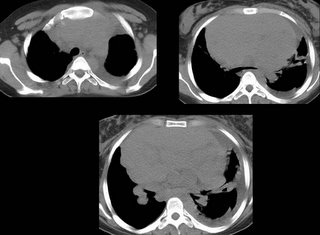
Pulmonary infiltrates
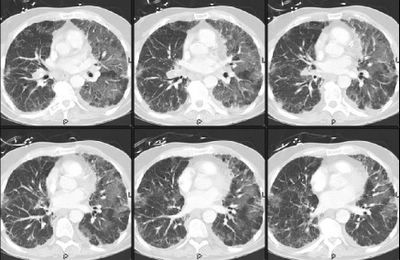
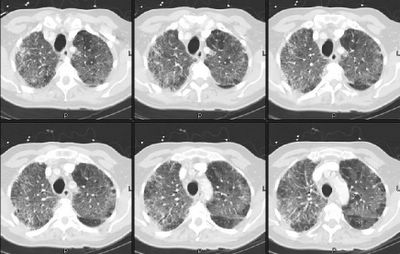
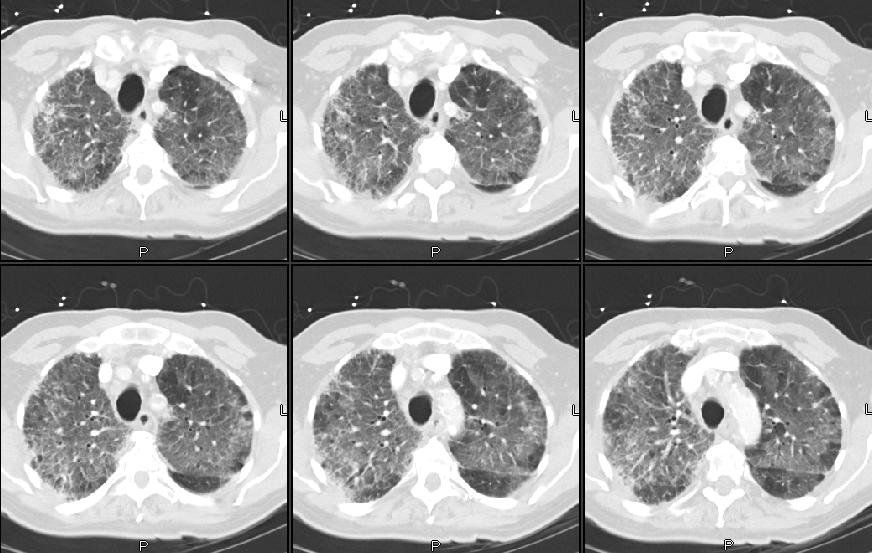
This is a 68 y/o man with a very remote TOB Hx (quit >20 years ago) who had an interesting initial presentation of persistent neck adenopathy since 1995. He had had many non-diagnostic biopsies over the years and was treated for toxo. He finally had an excisional Bx of an 8x6 cm neck node and was found to have Hodgkin's. He had mediastinal adenopathy at the time (7/05) and has received 3 cycles of ABVD. He was set up for another cycle in early December but presented to the hospital with worsening dyspnea, cough (non-productive) and fatigue and was found to be hypoxemic. He is not neutropenic but is quite hypoxic and I have posted his CxR and CT chest below.
What is your DDx and what would you do next?

What is your DDx and what would you do next?


Monday, December 19, 2005
Abnormal CT scan
This is an 83 y/o man sent to us by our CT surgeons. Two months ago he had a tracheo-bronchitis treated by his PCP. A CxR showed a subtle abnormality on his L lung and that was better seen on a CT scan. He is now assymptomatic but has a persistent abnormality on his L lung on a repeat CT scan (see below, this was done roughly 6 weeks after the first one).
He is a former smoker (quit in 1967) with no other remarkable exposures.
Exam is fairly normal.
PFTs showed mild COPD (FEV1~70% with normal TLC, increased RV and DLCO ~60%).
The surgeons thought we might want to see him before cutting anything out.
What would you do next?
He is a former smoker (quit in 1967) with no other remarkable exposures.
Exam is fairly normal.
PFTs showed mild COPD (FEV1~70% with normal TLC, increased RV and DLCO ~60%).
The surgeons thought we might want to see him before cutting anything out.
What would you do next?

Friday, December 16, 2005
Levalbuterol
Our hospital has a very high usage of levalbuterol as opposed to racemic albuterol (most of it actually not motivated by pulmonary). It is often prescribed in higher frequency than the q8 hour use. Pharmacy has been trying to rein this in because of cost differences.
There is a lot of data available (some conflicting) and most of it sponsored by Sepracor (such as Truitt's paper on Chest 2003).
What is your opinion on the use and have you noticed similar patterns with levalbuterol?
There is a lot of data available (some conflicting) and most of it sponsored by Sepracor (such as Truitt's paper on Chest 2003).
What is your opinion on the use and have you noticed similar patterns with levalbuterol?
Thursday, December 15, 2005
Follow up to lung mass
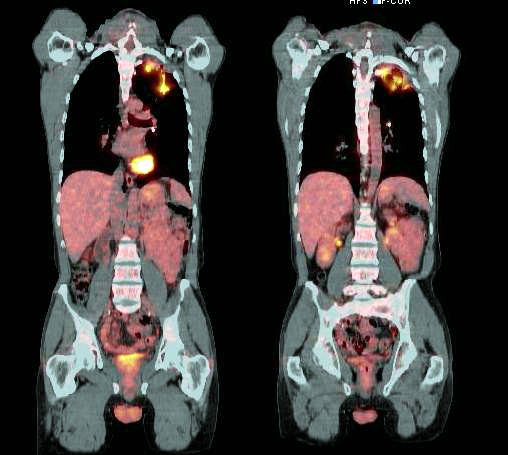
This is the man with the large LUL mass and the hot spot on the sacrum seen on PET. The main question was what to do and how to finish his staging. Our CT surgeon offered to do a mediastinoscopy for further staging (of a IIIA vs IIIB) to help decide on whether he would be operable. He had tumor invasion of the mediastinum itself (T4) with positive N2 nodes (IIIB). We are performing a MRI of the pelvis today to better define that hot spot (his PSA is high too) and a MRI of his head. Since he is not operable we feel inclined to further image but not biopsy the sacral lesion at this point. What do you think?
Wednesday, December 14, 2005
Bronchs and coag's
This comes up fairly often in patients with AFib, mechanical heart valves and liver disease who need bronch's. What is your comfortable cutoff for PT-INR and or platelets when doing a bronchoscopy? Is there any good data on safety and cutoff levels?
Ethical question
69 yo male with PMH of hypertension, CAD and DM2 presented to his PCP with fatigue and "falling asleep anywhere." After testing him for anemia, renal disease and thyroid disease, he decided to get a sleep study. The sleep study was grossly positive with an AHI (RDI) of 67 that occurred with both REM and NREM sleep. During the split night portion of the study, his AHI was reduced to 12 with CPAP of 11 cm H20.
He saw me after the study. When asked, he claimed to fall asleep reading the newspaper in the morning on the weekends, watching TV at night and had, on 2 occassions, fallen asleep while driving. He pulled over, napped for 10 minutes and started to drive again. There were no accidents and he needs to drive each day to get to work. He is constantly sleepy while driving and usually drives with the windows down in 20 degree temperatures to keep himself awake.
From our office, we arranged for CPAP to be delivered to his house the day of his appointment.
Would you ask him not to drive? If so, for how long?
Would you report this to the state (this is not required in the state of Michigan).
He saw me after the study. When asked, he claimed to fall asleep reading the newspaper in the morning on the weekends, watching TV at night and had, on 2 occassions, fallen asleep while driving. He pulled over, napped for 10 minutes and started to drive again. There were no accidents and he needs to drive each day to get to work. He is constantly sleepy while driving and usually drives with the windows down in 20 degree temperatures to keep himself awake.
From our office, we arranged for CPAP to be delivered to his house the day of his appointment.
Would you ask him not to drive? If so, for how long?
Would you report this to the state (this is not required in the state of Michigan).
Tuesday, December 13, 2005
Lung mass
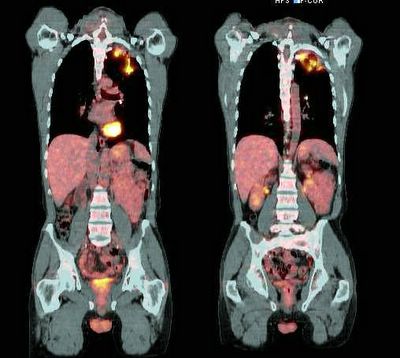
This is a man in his 60's with no previous lung or heart disease. He presented to the ER with atypical R-sided CP, had an abnormal CxR and had the following CT:
 I saw him in our office, he has an occasional cough and normal PFTs.
I saw him in our office, he has an occasional cough and normal PFTs.
I did a bronch which showed no endobronchial lesions but confirmed a NSCLCa (squamous).
His PET scan showed obvious uptake by the mass and an ipsilateral node.
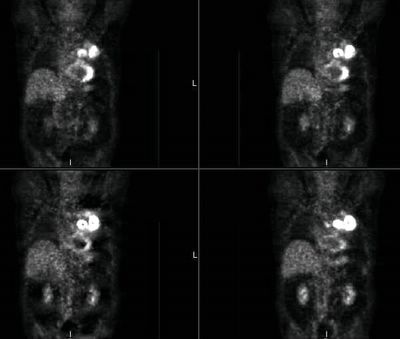 It also showed some increased uptake in the sacrum:
It also showed some increased uptake in the sacrum:
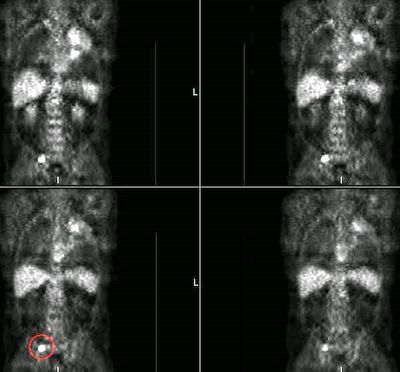 The sacral area is anterior and not approachable by CT-guided Bx... What would you do next? With the PET but no tissue confirmation from the sacrum would you consider him a stage IV? Would you try and get a surgical Bx from the sacrum?
The sacral area is anterior and not approachable by CT-guided Bx... What would you do next? With the PET but no tissue confirmation from the sacrum would you consider him a stage IV? Would you try and get a surgical Bx from the sacrum?
I did a bronch which showed no endobronchial lesions but confirmed a NSCLCa (squamous).
His PET scan showed obvious uptake by the mass and an ipsilateral node.
Monday, December 12, 2005
PET and SUV
new comment in unusual configuration cxr. I had a long discussion with the radiologist in nuclear medicine. He essentially refused to tell me the SUV value on a PET scan, saying that there was so much overlap that it was useless. He was not (yet) able to cite any references to back this up but will hopefully be getting back to me on this. Judging by some of the comments here, I gather some of you rely on this value when making decisions regarding the "hotness" of a lesion. While we are awaiting the radiologist's reply, is anyone aware of studies debunking/invalidating the utility of the SUV value?
Friday, December 09, 2005
Follow up to abnormal CT scan
This is the young guy with the mediastinal adenopathy. I did request a PET scan and there was no abnormal uptake anywhere. Mike L raised a good point on that discussion about PET-negative slow growing lymphomas. With these results, what would you do next?
Wednesday, December 07, 2005
rEmerson Biguns
19 year old woman who is 26 weeks pregnant presented with 2 weeks of progressive shortness of breath, which was worse lying down and better sitting up and leaning forward. + wheezing. No fever/chills/sweats. No weight loss. No cough/sputum production.
No past medical history/social history/family history of significance.
The exam was notable only for inspiratory and expriatory wheezing.
No past medical history/social history/family history of significance.
The exam was notable only for inspiratory and expriatory wheezing.

Monday, December 05, 2005
Abnormal CT scan
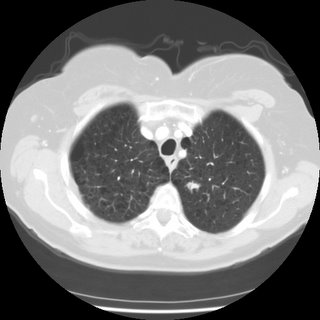
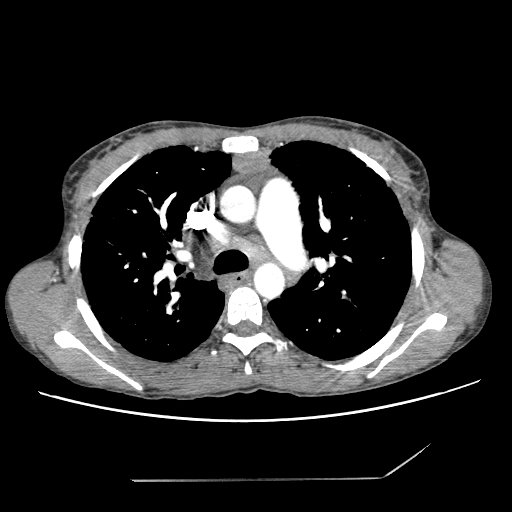
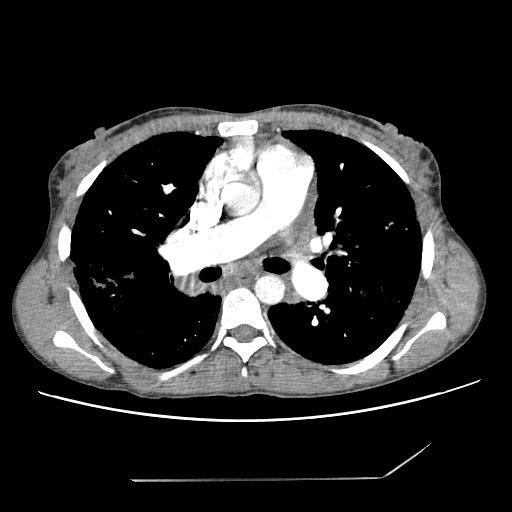
This is a 44 y/o man referred to our office because of an abnormal CT scan of the chest. He had fallen of a horse and had a CT scan of his thoracic spine and the mediastinal findings were incidental. He has NO respiratory symptoms. He is a smoker (1-1.5 pack/day x ~30years) and has normal PFTs. I have outlined the abnormality on the first cut so you may follow along. No other parenchymal abnormalities were noted.

How would you (or would you) work up this lesion?

How would you (or would you) work up this lesion?
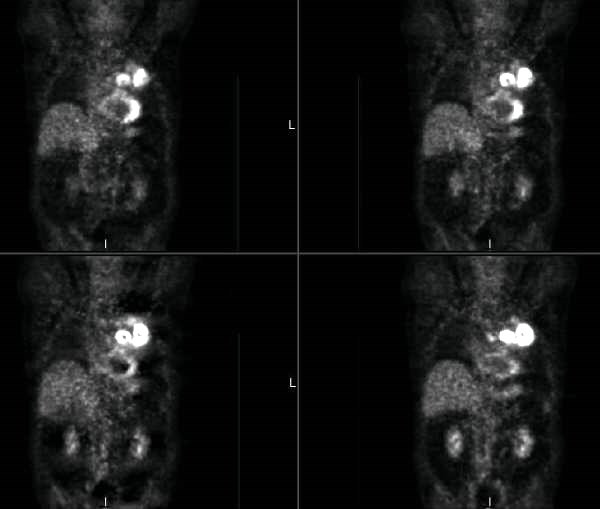
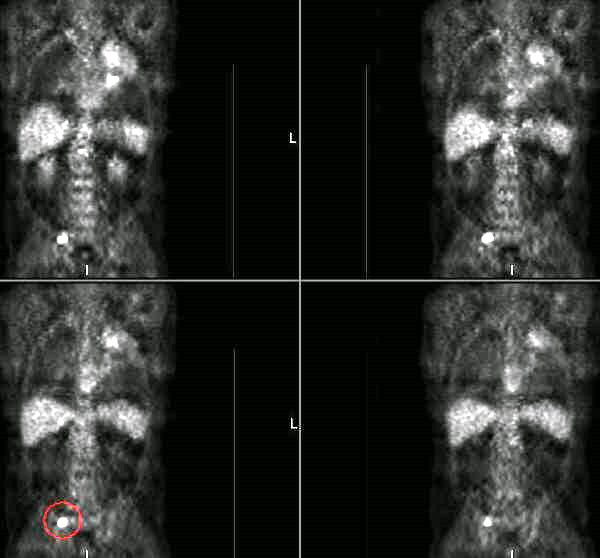
Interesting configuration of a lung lesion.
73-year-old female with mild COPD, former smoker. Found to have a left upper lobe nodule on x-ray:
 A CT scan was performed, confirming a 3 cm vertically oriented cylindrical lesion.
A CT scan was performed, confirming a 3 cm vertically oriented cylindrical lesion.

Do you agree that this is an unusual configuration for a malignancy? Could it be a mucous plug? Well, how about the fact that this is the PET scan results:

 A CT scan was performed, confirming a 3 cm vertically oriented cylindrical lesion.
A CT scan was performed, confirming a 3 cm vertically oriented cylindrical lesion.

Do you agree that this is an unusual configuration for a malignancy? Could it be a mucous plug? Well, how about the fact that this is the PET scan results:

Friday, December 02, 2005
Update on previous lung cancer
There were no comments on this case but I would still like to hear your suggestions since it is an ongoing case and I don't have a final answer yet. This is the 61 y/o man with the previous IIB NSCLCa now with abnormal hilum and RML bronchus with path changes of radiation but no obvious malignancy. As it is getting close to the holidays, he came to the office yesterday for the bronch results and we agreed to watch him closely with a repeat CT in 3 months and no other invasive procedures. What would you do?
Update on lung mass
This is the 54 y/o man with >85p/y of TOB and the PET+ lung mass. We felt that with his pre-test likelihood of malignancy, surgery was his best option. He underwent a LULobectomy with partial resection of ribs as the mass was adherent to them (no bone involvement on the PET-CT) and the frozen was "consistent" with adenoCa. The final path was a granulomatous inflammatory mass with fungal agents consistent with blasto and no cancer.
Update on abnormal CxR and hypoxemia
This is the 58-year-old white male with the ICD, and pulmonary infiltrates. Good pick up on the Amio (I thought about just listin "antiarrhythmics" but that seemed unfair). We followed along the same ideas posted: gentle diuresis, continued BiPAP and then a bronch. He had alveolar spaces filled with foamy macs full of phospholipid complexes. Amio was discontinued and he was placed on steroids. He went to a SNF and eventually came off O2. His PFTs normalized and his CxR cleared up.

Thursday, December 01, 2005
Update on ongoing cases
We have three cases from this week and one question/comment going on and still need to hear from our readers. Try and leave comments/suggestions and we will be posting the conclusions to the lung mass cases tomorrow.
Previous lung cancer
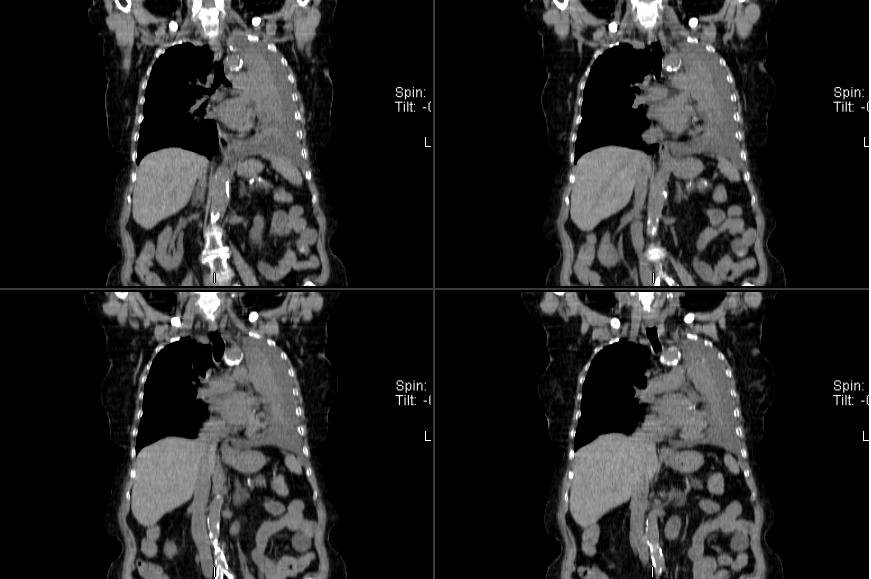
This is a 61 y/o man who was seen in our office last year. He had significant obesity and OSA and was found to have a RUL mass. He underwent resection of a IIB (T2N1M0) NSCLCa (squamous), followed by xRt and chemoTx. His course since then has been remarkable for a fall and a hip Fx but no respiratory problems.
He came back to his PCP this past month with a new cough and R chest tightness. His CT showed some loss of volume and more soft tissue swelling in the hilar area (see below):
Incidentally he had this huge gallstone (cool pic):
I bronch'ed him and he had narrowing and scarring of the residual RML bronchus with normal RLL and a healthy looking RUL stump. EndoBBx, brushings and lavages were remarkable for radiation changes and atypia but no neoplasm. Would you do a PET, a more invasive sampling (e.g. Mediastinoscopy) or just follow him after some ABTx since he has already had maximal therapy to the area and would have limited options with recurrent Ca?
He came back to his PCP this past month with a new cough and R chest tightness. His CT showed some loss of volume and more soft tissue swelling in the hilar area (see below):

Incidentally he had this huge gallstone (cool pic):
I bronch'ed him and he had narrowing and scarring of the residual RML bronchus with normal RLL and a healthy looking RUL stump. EndoBBx, brushings and lavages were remarkable for radiation changes and atypia but no neoplasm. Would you do a PET, a more invasive sampling (e.g. Mediastinoscopy) or just follow him after some ABTx since he has already had maximal therapy to the area and would have limited options with recurrent Ca?
Wednesday, November 30, 2005
Lung mass
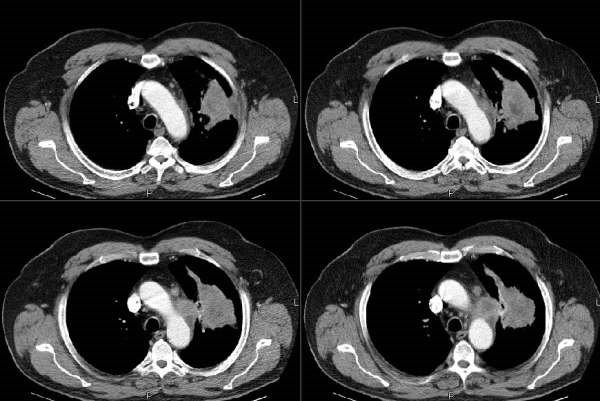
This is a 54 y/o man with a 2-pack day TOB habit who had been referred to us for atypical chest pain. He complained of intermittent chest tightness and had had a negative cardiac w/up (normal SPECT-stress, normal EF, etc.). We identified a mild to moderate obstructive ventilatory deffect (normal FVC and FEV1 that fluctuated between high 50s to 70%) and started him on bronchodilators and continued to counsel him about smoking. He had a CxR with a RUL bulla and some L apical scarring. In the course of his follow-up however, we performed a repeat CxR which revealed a new LUL lesion:

He had some cough at the time so he was given a course of ABTx and followed closely and there was no improvement in the lesion after 4 weeks. A CT scan was obtained and revealed a soft tissue mass associated with some scarring:
A bronch was done and was non-diagnostic and the mass remained unchanged on CxR.
A PET-CT was then performed and revealed intense uptake on the area (SUV ~5.7 about 6 weeks after he had completed the course of ABTx) :
What would you do next?

He had some cough at the time so he was given a course of ABTx and followed closely and there was no improvement in the lesion after 4 weeks. A CT scan was obtained and revealed a soft tissue mass associated with some scarring:

A bronch was done and was non-diagnostic and the mass remained unchanged on CxR.
A PET-CT was then performed and revealed intense uptake on the area (SUV ~5.7 about 6 weeks after he had completed the course of ABTx) :
What would you do next?
Tuesday, November 29, 2005
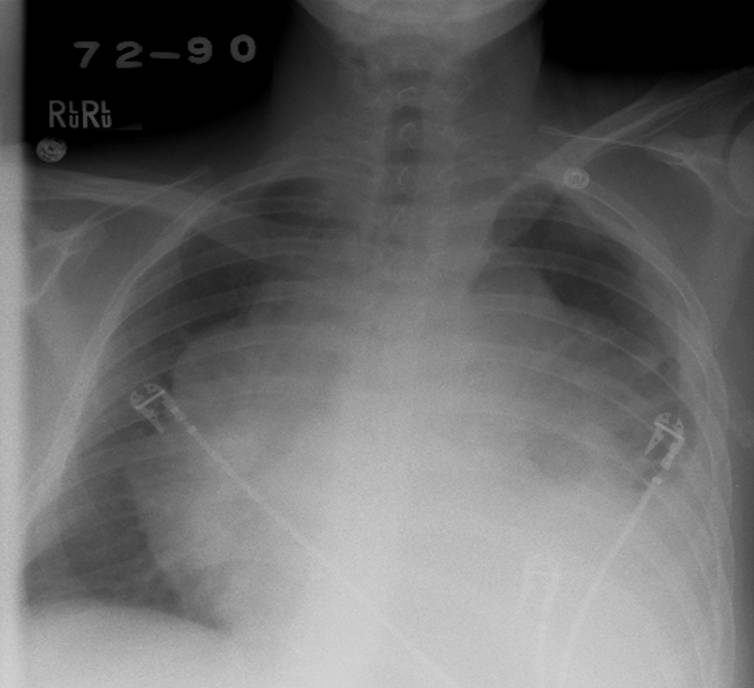
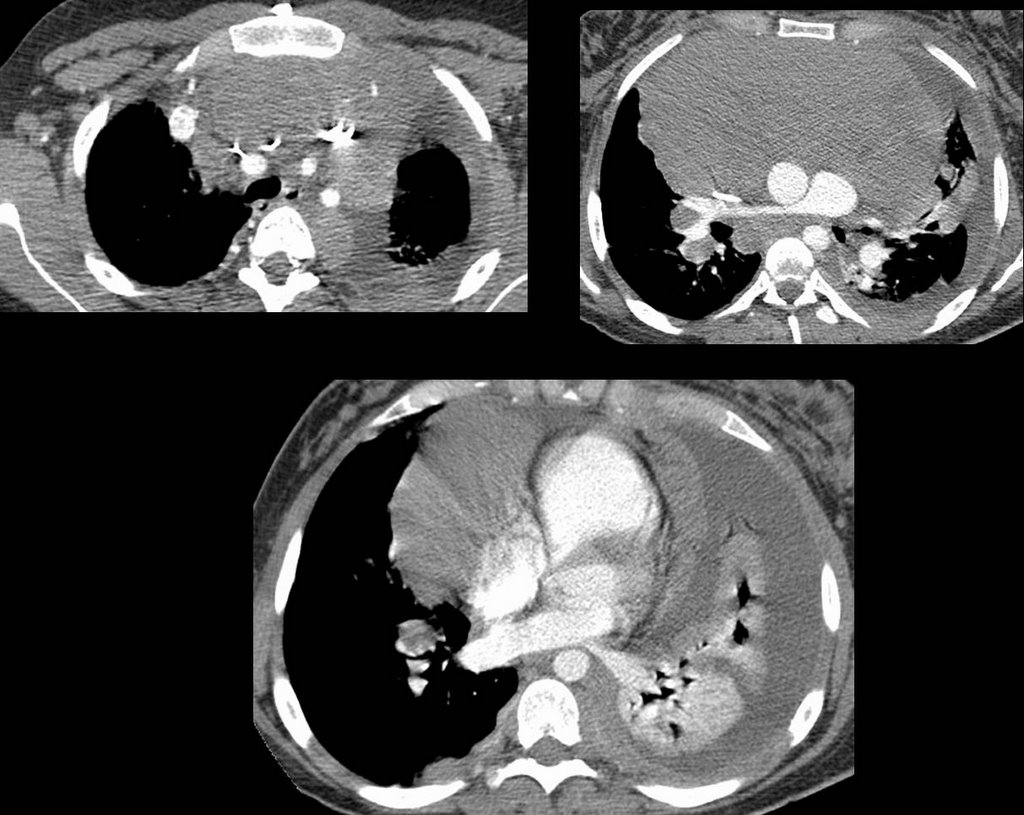
Abnormal CxR and hypoxemia
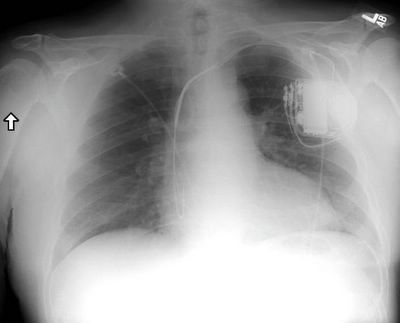
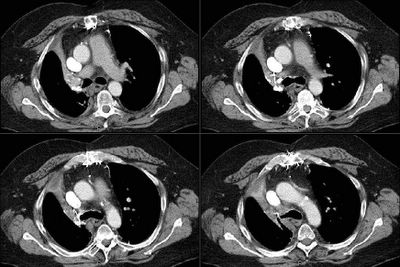
We were consulted on this pleasant 58-year-old white male with known coronary artery disease. He was last admitted 3 months ago with a inferior lateral wall myocardial infarction. He is status post angioplasty. He has a history of chronic obstructive pulmonary disease. He had been doing fairly well andhad gone back to work as an electrician however, over the last five days he developed increasing lethargy, chills and felt feverish with a dry nonproductive cough and worsening dyspnea.
PMHx: Ventricular tachycardia, S/P AICD/PM. CAD, S/P inferior lateral myocardial infarction and previous EF~45%. He is status post stenting of the OM/circumflex. Chronic obstructive pulmonary disease. Dyslipidemia.
Current meds: Lovenox, Albuterol and Atrovent, Levofloxacin, Aspirin and Amiodarone.
FHx: Noncontributory
SHx: Heavy cigarette smoker, he quit 3 months ago. He has been drinking several beers daily. He works as an electrician. He lives alone and his wife died last year.
ROS non-contributory.
On exam he was tachypneic to 36 with an O2Sat of 90% on BiPAP with 100% FiO2. BP and HR were stable. His lungs had very faint crackles and no wheezing or ronchi.
ABG was: 7.43/CO2: 37/ O2: 58 on 100% FM.
His CxR and CT are posted below.
What would you do next?



PMHx: Ventricular tachycardia, S/P AICD/PM. CAD, S/P inferior lateral myocardial infarction and previous EF~45%. He is status post stenting of the OM/circumflex. Chronic obstructive pulmonary disease. Dyslipidemia.
Current meds: Lovenox, Albuterol and Atrovent, Levofloxacin, Aspirin and Amiodarone.
FHx: Noncontributory
SHx: Heavy cigarette smoker, he quit 3 months ago. He has been drinking several beers daily. He works as an electrician. He lives alone and his wife died last year.
ROS non-contributory.
On exam he was tachypneic to 36 with an O2Sat of 90% on BiPAP with 100% FiO2. BP and HR were stable. His lungs had very faint crackles and no wheezing or ronchi.
ABG was: 7.43/CO2: 37/ O2: 58 on 100% FM.
His CxR and CT are posted below.
What would you do next?


Monday, November 28, 2005
ICS in COPD
This is a quick question. How often do you add inhaled steroids in the care of your COPD patients? I am more curious about people's anecdotal and personal opinions rather than data (FEV1< 30%, response to PO steroid trial, etc.).
Thursday, November 24, 2005
Tuesday, November 22, 2005
Follow-up to Picture Friday (Janeway lesions)
This is the 65 y/o man with FUO and palmar and plantar lesions. He has now had about 4 weeks of ABTx. His serologies for Coxiella and RMSF (and other Rickettsia) have been negative. His TEE showed some abnormal signal at one of his pacer leads but no vegetations. He remains afebrile, his Janeway lesions and splinter hemorrhages are almost completely gone and his arthralgias resolved. A Bx of one of his lesions was read as embolic infectious vasculitis. We still don't have an organism but with his good clinical response I have called it "culture-negative endovascular infection" and he will have a total of 6 weeks of therapy because of the hardware (PM). Any other ideas?
Monday, November 21, 2005
Consult to "bronch"
We were asked to consult on a patient to "rule out endobronchial lesion via bronch".
A 52-year-old male has an unremarkable past medical history. He has a 100 pack-year histor and is an alcoholic. He noticed a "boil" over his "right collar bone". He thought maybe he was bitten by an insect. Since then has had progressivesymptoms resulting in chest pain and difficulty breathing.
Blood pressure 120/70, heart rate 120, respiratory rate 22, temperature 36.4. 99% on four liters nasal cannula. General appearance: This is a cachectic male. Lungs sounds were significant for good air entry bilaterally with vesicular breath sounds, no rhonchi or wheeze appreciated. Cardiovascular significant for a tachycardia. otherwise unremarkable. b Over the mid sternum at around T3 is a 1 cm round red maculopapular lesion; no pus from the site.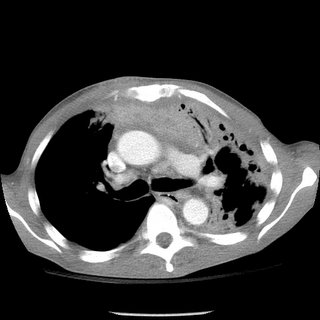

A 52-year-old male has an unremarkable past medical history. He has a 100 pack-year histor and is an alcoholic. He noticed a "boil" over his "right collar bone". He thought maybe he was bitten by an insect. Since then has had progressivesymptoms resulting in chest pain and difficulty breathing.
Blood pressure 120/70, heart rate 120, respiratory rate 22, temperature 36.4. 99% on four liters nasal cannula. General appearance: This is a cachectic male. Lungs sounds were significant for good air entry bilaterally with vesicular breath sounds, no rhonchi or wheeze appreciated. Cardiovascular significant for a tachycardia. otherwise unremarkable. b Over the mid sternum at around T3 is a 1 cm round red maculopapular lesion; no pus from the site.


Thursday, November 17, 2005
Cool films!
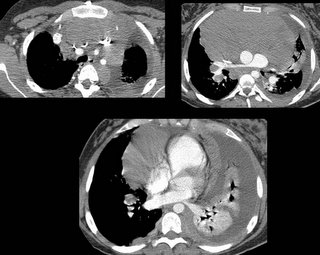
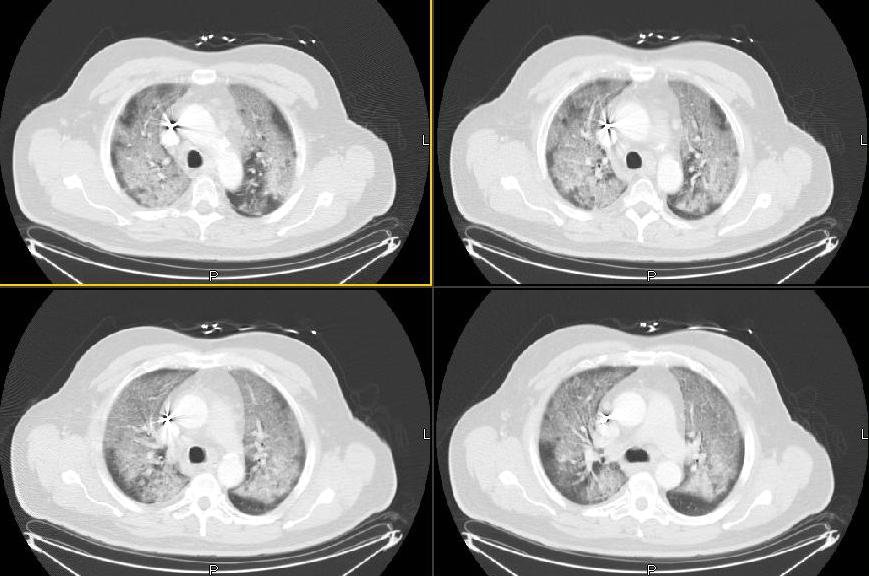
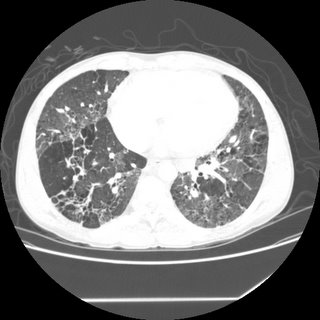
50-something y/o man with no significant past medical history prior to 3-4 months ago, when he developed progressive shortness of breath and required oxygen treatment. His evaluation elsewhere led to a diagnosis of BOOP on a surgical lung biopsy, and he was started on steroids-initially 20mg/day. He failed to improve, and a few weeks later his prednisone was bumped to 40mg/day, and then a few weeks later he had still failed to improve and his dose was increased to 60 mg/day.
A few weeks later, he was admitted to another hospital with continued dyspnea, and transferred to our institution, where he quickly developed respiratory distress. The following CT scan was obtained, and he was transferred to the ICU.
Questions:
1) What intervention led to a rapid improvement in this patients acute respiratory decompensation.
2) What is the the differential diagnosis for the other two findings on this CT scan
3) What steps would you take to further evaluate and treat the patient?
A few weeks later, he was admitted to another hospital with continued dyspnea, and transferred to our institution, where he quickly developed respiratory distress. The following CT scan was obtained, and he was transferred to the ICU.
Questions:
1) What intervention led to a rapid improvement in this patients acute respiratory decompensation.
2) What is the the differential diagnosis for the other two findings on this CT scan
3) What steps would you take to further evaluate and treat the patient?
Wednesday, November 16, 2005
Followup to 2 weeks of dyspnea
Mendez and Jeff H both picked up on the salient points. Here is the canned message from Carlos as he hangs out somewhere in Lima:
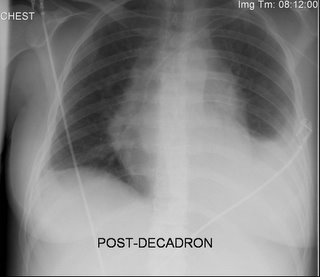
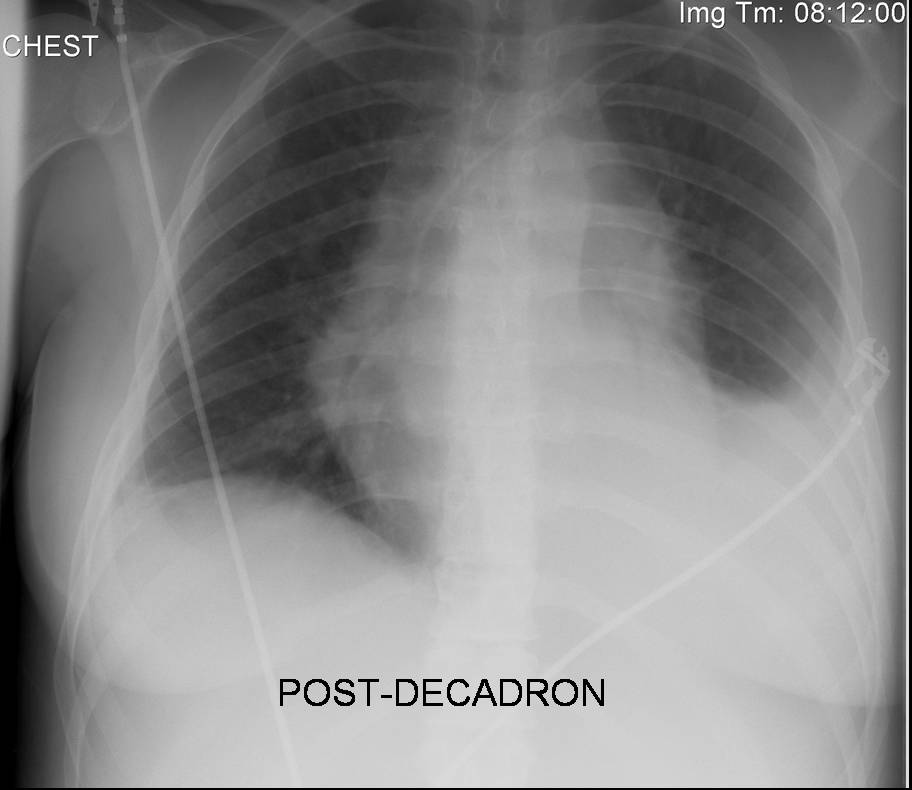
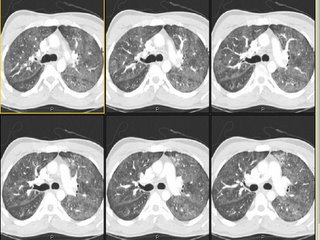
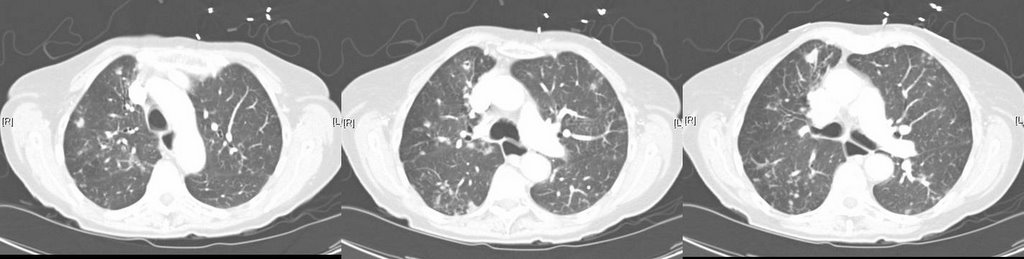
For those who picked up on the "clear lungs" with all the ground-glass we also suspected PCP in this young man with no other Hx of structural lung Dz. He was admitted at night so we started him on IV bactrim and steroids (and a 3 rd gen Cef), ordered a rapid HIV test and planned on doing a bronch. His HIV was positive and then they volunteered his partner was HIV+ and requested a transfer to a University Hospital here in TN. His PCP DNA PCR was positive, his CD4 was around 50 and overall he did very well. Here is his follow-up CxR:
For those who picked up on the "clear lungs" with all the ground-glass we also suspected PCP in this young man with no other Hx of structural lung Dz. He was admitted at night so we started him on IV bactrim and steroids (and a 3 rd gen Cef), ordered a rapid HIV test and planned on doing a bronch. His HIV was positive and then they volunteered his partner was HIV+ and requested a transfer to a University Hospital here in TN. His PCP DNA PCR was positive, his CD4 was around 50 and overall he did very well. Here is his follow-up CxR:

ARDS and pulmonary function
From a PCP in NC:
"Quick question: what PFT parameter is the last to normalize (if it ever does) in patients with ARDS, 1 year out?" The pulmonary boards were yesterday so some of you fellows out there should have no problem with this question.....
"Quick question: what PFT parameter is the last to normalize (if it ever does) in patients with ARDS, 1 year out?" The pulmonary boards were yesterday so some of you fellows out there should have no problem with this question.....
Tuesday, November 15, 2005
2 weeks of dyspnea
Carlos' case:
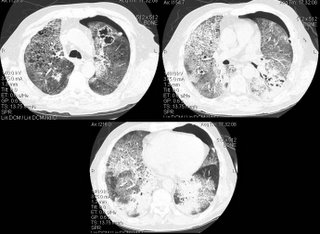
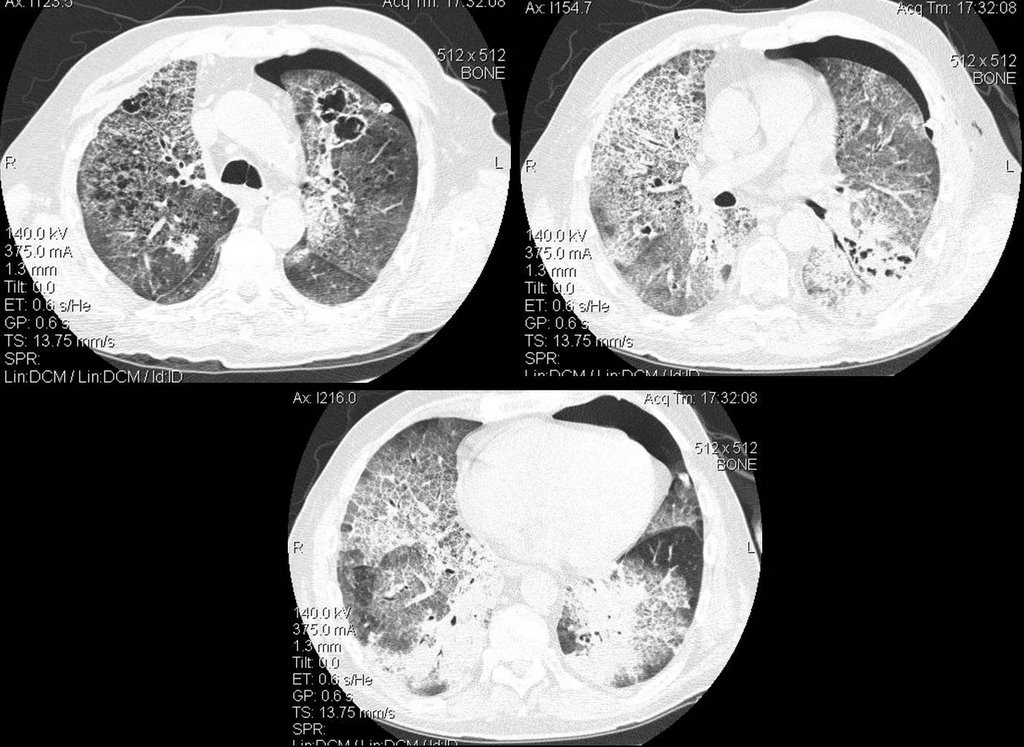
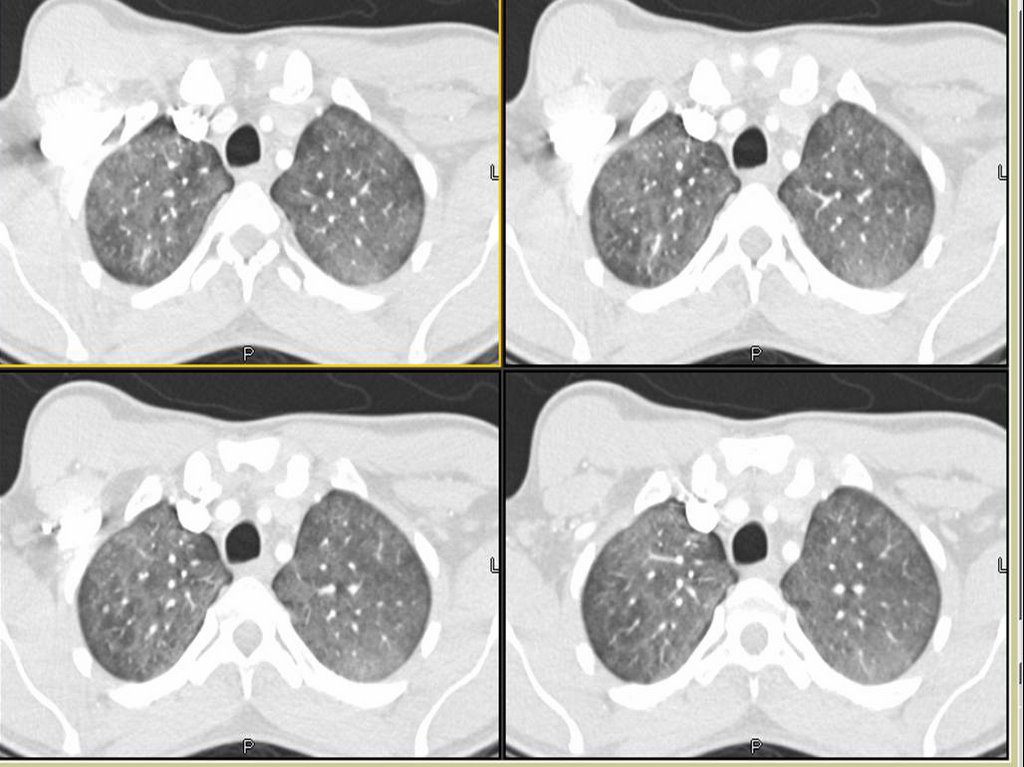
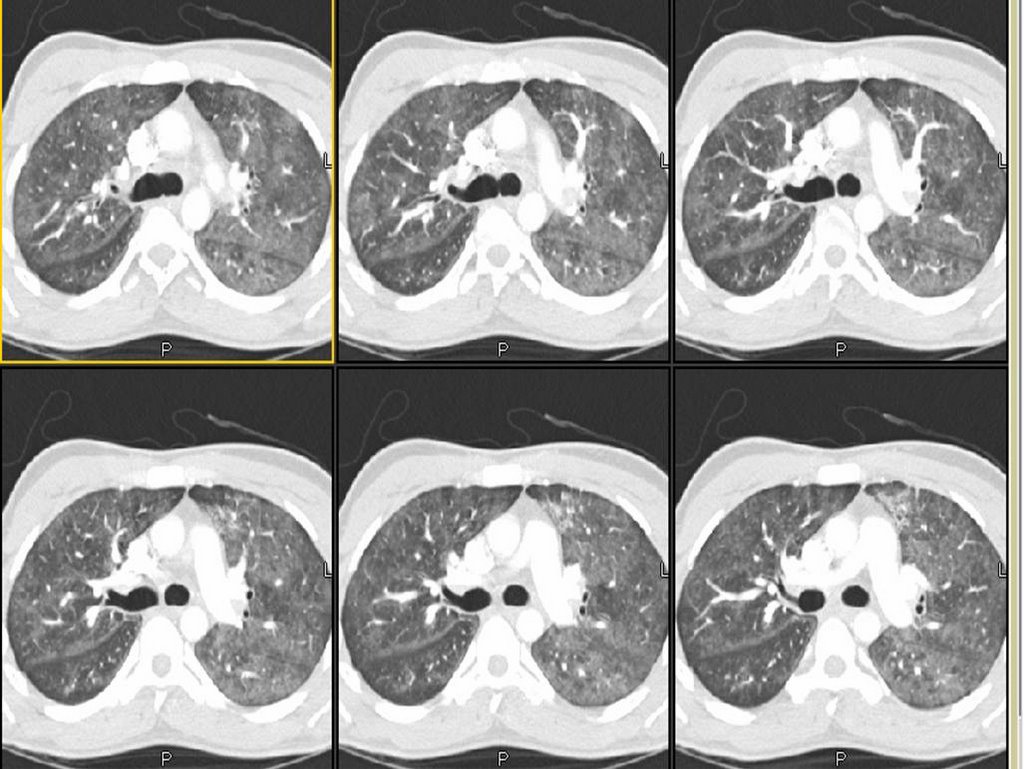
We were consulted on this is a 28 y/o man with no previous PMHx who presented to the ER with progressive worsening DOE over the past 2-3 weeks with some dry cough. Occasional chills but no fevers or night sweats. In the ER he was febrile and hypoxic (7.47/33/58) and was admitted for further care.
PMHx: No lung Dz.
SHx: Occasional ETOH, TOB 1ppd x 10 years, no occupational exposures, no IVDA, lives with same-sex partner.
On exam, AAOx3 in minimal resp discomfort. Clear lungs B/L. S1/S2 RRR and benign abdomen.
CxR:

The ER did a CT-angio (on everybody), which showed no PE but the following changes:
What is your DDx and what would you do next?
We were consulted on this is a 28 y/o man with no previous PMHx who presented to the ER with progressive worsening DOE over the past 2-3 weeks with some dry cough. Occasional chills but no fevers or night sweats. In the ER he was febrile and hypoxic (7.47/33/58) and was admitted for further care.
PMHx: No lung Dz.
SHx: Occasional ETOH, TOB 1ppd x 10 years, no occupational exposures, no IVDA, lives with same-sex partner.
On exam, AAOx3 in minimal resp discomfort. Clear lungs B/L. S1/S2 RRR and benign abdomen.
CxR:

The ER did a CT-angio (on everybody), which showed no PE but the following changes:
What is your DDx and what would you do next?
Monday, November 14, 2005
Pulmonary embolism and intervention
The cover of the Nov 1st Blue journal (AJRCCM 172(9)) showing a fibrosed thrombus reminded me how controversial treatment of this entity can be. I was interested in what others felt about the following. We all know that no study has demonstrated a change in mortality after thrombolytic therapy for acute massive PE. We also know that some of the beneficial paramters (such as right heart strain or PA pressure) are no different than just IV heparin after about 7 days. Nonetheless, does anyone feel that the lack of a mortality benefit may be as a result of the studies being underpowered? If this is the case, perhaps thrombolytics should be used as default pending a larger study (for massive PE without obvious bleeding risks). On the other hand, if the concensus is that nothing is proven with regards to mortality and thus thrombolytics are NOT indicated by default until that larger study comes along, should we ever administer it?
Now it gets even more sketchy when we consider surgical embolectomy. When do you consider this intervention? Some have argued that it absolutely has no place. Others will ship everyone with a b/l saddle embolus out to the Mayo for embolectomy.
I think there is not a lot of convincing data out there for anything other than good old fashioned anticoagulation and IV fluids (and some prayer).
What do you all do when you get the call about a patient with acute massive P.E.?
Now it gets even more sketchy when we consider surgical embolectomy. When do you consider this intervention? Some have argued that it absolutely has no place. Others will ship everyone with a b/l saddle embolus out to the Mayo for embolectomy.
I think there is not a lot of convincing data out there for anything other than good old fashioned anticoagulation and IV fluids (and some prayer).
What do you all do when you get the call about a patient with acute massive P.E.?
Sunday, November 13, 2005
When to Treat MAI
80 yo female with PVOD s/p TIA many years ago presented with multiple pulm nodules about 2 years ago to her PCP. The radiologist was worried about TB at the time, so she was sent to the county health clinic. The CT also showed evidence of broniectasis at that time. Sputum cultures revealed MAI.
She went to an ID doc, who convinced her the treatment is worse than the disease. So, she opted for no treatment.
She is pretty much asymptomatic since 1/04 (the time of her original CT), but she presented to the ER with hemoptysis (about 5 tbsp, bloody sputum with clots). She was watched in observation overnight and it did not recur.
Her repeat CT scan (to rule out PE, of course), showed stable nodules. There were more of them, but the ones visualized 2 years ago are definitively stable.

Would you offer a bronch, or is the CT with bronchiectasis enough to convince you of the diagnosis (she has never before been endoscopically evaluated)?
Would you treat the MAI in this 80 yo, relatively asymptomatic individual?
She went to an ID doc, who convinced her the treatment is worse than the disease. So, she opted for no treatment.
She is pretty much asymptomatic since 1/04 (the time of her original CT), but she presented to the ER with hemoptysis (about 5 tbsp, bloody sputum with clots). She was watched in observation overnight and it did not recur.
Her repeat CT scan (to rule out PE, of course), showed stable nodules. There were more of them, but the ones visualized 2 years ago are definitively stable.
Would you offer a bronch, or is the CT with bronchiectasis enough to convince you of the diagnosis (she has never before been endoscopically evaluated)?
Would you treat the MAI in this 80 yo, relatively asymptomatic individual?
Tuesday, November 08, 2005
COPD and weight loss.
From Carlos, who is on vacation:
This is a 60 y/o man with a 50 p/y Hx of smoking sent to us because of worsening DOE, cough productive of scant amounts of thick sputum and weight loss. No hemoptysis, no CP.
PMHx: Mild HTN.
SHx: 50 p/y TOB. Quit in 2003.
On exam, thin male in NAD. Distant BS B/L with rare R upper crackles. S1/S2 RRR, benign abdomen.
His Spiro revealed an FEV1 of 1.1 L (27% of his predicted) and he had the following CxR and CT scan findings:

update(after 1st 2 comments):
He was started on aggressive bronchodilator therapy, given ABTx and steroids and returned with symptomatic improvement. His FEV1 increased to 2.17L (53%) and he felt better. However, he still had some weight loss (6 lbs.) and a persistent infiltrate after 4 weeks. I did a bronch which revealed only chronic bronchitis and no other Dx.
A PET-CT was done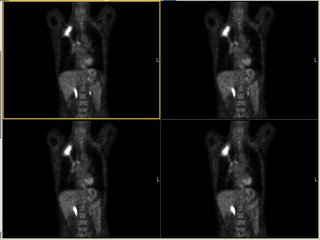 and it revealed marked FDG uptake to the RUL (average SVU of 13 with max SVU of 21) and nowhere else. What would you do next?
and it revealed marked FDG uptake to the RUL (average SVU of 13 with max SVU of 21) and nowhere else. What would you do next?
This is a 60 y/o man with a 50 p/y Hx of smoking sent to us because of worsening DOE, cough productive of scant amounts of thick sputum and weight loss. No hemoptysis, no CP.
PMHx: Mild HTN.
SHx: 50 p/y TOB. Quit in 2003.
On exam, thin male in NAD. Distant BS B/L with rare R upper crackles. S1/S2 RRR, benign abdomen.
His Spiro revealed an FEV1 of 1.1 L (27% of his predicted) and he had the following CxR and CT scan findings:

update(after 1st 2 comments):
He was started on aggressive bronchodilator therapy, given ABTx and steroids and returned with symptomatic improvement. His FEV1 increased to 2.17L (53%) and he felt better. However, he still had some weight loss (6 lbs.) and a persistent infiltrate after 4 weeks. I did a bronch which revealed only chronic bronchitis and no other Dx.
A PET-CT was done
 and it revealed marked FDG uptake to the RUL (average SVU of 13 with max SVU of 21) and nowhere else. What would you do next?
and it revealed marked FDG uptake to the RUL (average SVU of 13 with max SVU of 21) and nowhere else. What would you do next?
Monday, November 07, 2005
18 year old with hemoptysis
18-year-old male referred for hemoptysis. He reports several episodes of pneumonia in last several years. His mother believes that these have all been on the "right chest." The most recent episode of pneumonia had occurred during the last football season, when he developed cough and hemoptysis. By report, he had an abnormal chest x-ray at that time. He was treated with antibiotics and reports that the symptoms resolved. He again had hemoptysis in a few months later. A PPD was negative. No images of a chest CT, but there was right middle lobe bronchiectasis.
Pmhx Status post hernia repair, rhinoplasty, right elbow surgery. In addition, the patient has a history of a racing heart and has been worked up for possible supraventricular tachycardia. In addition, the patient had a mole punch biopsied off his left back inferior to the scapula and does not know what the pathology for this showed.
SH: no alcohol, tobacco, or drug use
Physical Exam: His P is 49. BP is 108/57. His RR is 16, and his WT is 79 kg. In appearance, he is a well-developed, well- nourished young man in no distress. HEENT: Lymph node examination was no supraclavicular adenopathy. Pulmonary: clear to auscultation with both quiet and forced expiratory maneuvers from base to apex bilaterally. He is resonant to percussion throughout. Cardiac examination: Regular rhythm. S1 and S2 are of normal quality without murmur, gallop, or rub. He had no pedal edema, and he had 2+ radial pulses.
A bronch showd the following in the RML:
My collegue proceeded to evaluate further into the bronchus where they identified copious mucous and a foreign body. The foreign body was extracted with biopsy forceps. Under direct visualization it appeared to be a piece of organic green matter that resembled a branch tip of a pine tree.
Final diagnosis:
LUNG, RIGHT MIDDLE LOBE, BIOPSY:
1. BENIGN MARKEDLY INFLAMED BRONCHIAL MUCOSA AND FRAGMENTS OF
GRANULATION TISSUE.
2. FOREIGN MATERIAL CONSISTENT WITH VEGETABLE PARTICLE.
B. RIGHT LOBE, BIOPSY: FOREIGN BODY.
The patient breathed in a pine needle....
Pmhx Status post hernia repair, rhinoplasty, right elbow surgery. In addition, the patient has a history of a racing heart and has been worked up for possible supraventricular tachycardia. In addition, the patient had a mole punch biopsied off his left back inferior to the scapula and does not know what the pathology for this showed.
SH: no alcohol, tobacco, or drug use
Physical Exam: His P is 49. BP is 108/57. His RR is 16, and his WT is 79 kg. In appearance, he is a well-developed, well- nourished young man in no distress. HEENT: Lymph node examination was no supraclavicular adenopathy. Pulmonary: clear to auscultation with both quiet and forced expiratory maneuvers from base to apex bilaterally. He is resonant to percussion throughout. Cardiac examination: Regular rhythm. S1 and S2 are of normal quality without murmur, gallop, or rub. He had no pedal edema, and he had 2+ radial pulses.
A bronch showd the following in the RML:

My collegue proceeded to evaluate further into the bronchus where they identified copious mucous and a foreign body. The foreign body was extracted with biopsy forceps. Under direct visualization it appeared to be a piece of organic green matter that resembled a branch tip of a pine tree.
Final diagnosis:
LUNG, RIGHT MIDDLE LOBE, BIOPSY:
1. BENIGN MARKEDLY INFLAMED BRONCHIAL MUCOSA AND FRAGMENTS OF
GRANULATION TISSUE.
2. FOREIGN MATERIAL CONSISTENT WITH VEGETABLE PARTICLE.
B. RIGHT LOBE, BIOPSY: FOREIGN BODY.
The patient breathed in a pine needle....
Friday, November 04, 2005
Approach to this lesion
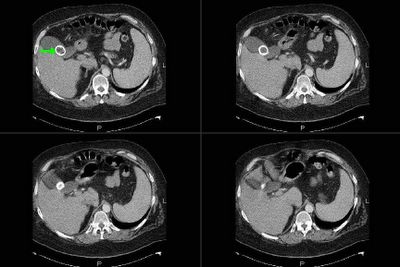
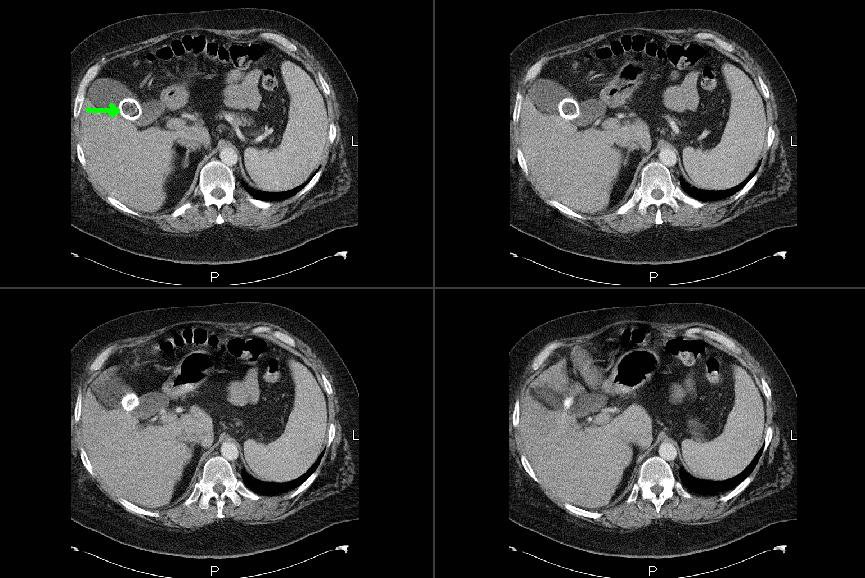
A physician wants some feedback regarding how to approach this lesion. This is an abdominal CT. A chest CT has not yet been done. The quesion regarding approach: get a PET? Go right to CT-guided biopsy? Get a full CT of chest first in case soemthign shows up that would make a bronch more helpful?
He's a patient with COPD and heavy smoking history. Abd CT was obtained b/c of some nausea.

He's a patient with COPD and heavy smoking history. Abd CT was obtained b/c of some nausea.

Thursday, November 03, 2005
Check out our ongoing cases!
Just a reminder to check on some of the ongoing cases.
DKeena had a great case on Enbrel-associated infiltrates in need of comments.
I have posted follow-ups to the drop in ETCO2 case (check out the CT) and the abnormal CxR as well as the presumed IE.
And we are looking forward to more info on Jennings' case with pancytopenia and abnormal lungs.
DKeena had a great case on Enbrel-associated infiltrates in need of comments.
I have posted follow-ups to the drop in ETCO2 case (check out the CT) and the abnormal CxR as well as the presumed IE.
And we are looking forward to more info on Jennings' case with pancytopenia and abnormal lungs.
Update on "update on picture Friday"
This is the 65 y/o man with FUO and palmar and plantar lesions posted on Picture Friday. There have been a few very good new comments on the original post. Dr Jon wrote:
Rickettsial infection: what about R. prowazekii? More common in elderly, and consistent with petechiae, but not common in US. Has he ever had typhus? There is Brill-Zinsser Disease (has he ever traveled outside th country?)Also about the endocarditis, maybe C. psittaci (hard/impossible to culture), does he have any birds?
He did not have birds and no exposures to suggest typhus. No recent travels. His serologies for Q fever, RMSF, Rickettsia prowazekii and Ehrlichia came back today and were all negative. He has remained afebrile and his Janeway lesions are resolving. A skin punch biopsy was interpreted as infectious embolic vasculitis though no organisms were seen. All Cxs remain negative. A TEE showed no veggies but there were some echo changes at the PM atrial lead site concerning for a small endocardial abcess. His CRP is down from 30 to 6 but now his Creatinine has crept up from <1.5>3%.
So we are still treating him for Cx- IE. Any other ideas?
Rickettsial infection: what about R. prowazekii? More common in elderly, and consistent with petechiae, but not common in US. Has he ever had typhus? There is Brill-Zinsser Disease (has he ever traveled outside th country?)Also about the endocarditis, maybe C. psittaci (hard/impossible to culture), does he have any birds?
He did not have birds and no exposures to suggest typhus. No recent travels. His serologies for Q fever, RMSF, Rickettsia prowazekii and Ehrlichia came back today and were all negative. He has remained afebrile and his Janeway lesions are resolving. A skin punch biopsy was interpreted as infectious embolic vasculitis though no organisms were seen. All Cxs remain negative. A TEE showed no veggies but there were some echo changes at the PM atrial lead site concerning for a small endocardial abcess. His CRP is down from 30 to 6 but now his Creatinine has crept up from <1.5>3%.
So we are still treating him for Cx- IE. Any other ideas?
Follow-up to abnormal CxR - part II
This is the woman in her 70s with an abnormal CxR. After the thoracentesis she had more L lung collapse: by the time of the bronch and the f/up PET she had complete L lung collapse (making her at least a IIIA). Her past showed uptake only in the peri-hilar mass itself. Our surgeons and a CT surgeon from a large University Center nearby felt that though she was a IIIA, her lesion was very proximal (less than 2 cm to the carina) and she would be a poor candidate for a pneumonectomy so she is receivin Chemo and xRt. She will follow-up with us and may benefit from APC or stenting to the lesion to improve drainage/clearance of the collapsed lung.
Wednesday, November 02, 2005
Unbound Medicine
We came across this jewel of a site from Mexico that focuses on medical education. As such there are some interesting cases posted there.
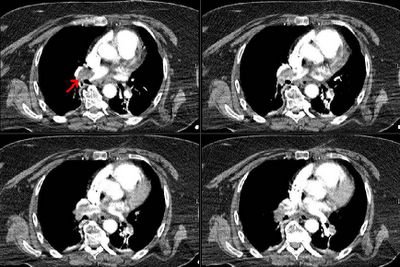
Follow-up to abnormal CxR
This is the woman in her 70s with an abnormal CxR. Everyone picked up on the loss of volume and nobody was "fooled" by the negative CT last year (it was really unremarkable). She had a CT scan seen below:


Most of her L lung was collapsed with a smallish effusion. Her effusion was exudative with negative cytology. I did a bronch and she had a NSCLCa occluding her L mainstem bronchus. Her Spiro (with her L lung collapsed) revealed an FEV1~ 800cc.
What would you suggest as the next step?
Most of her L lung was collapsed with a smallish effusion. Her effusion was exudative with negative cytology. I did a bronch and she had a NSCLCa occluding her L mainstem bronchus. Her Spiro (with her L lung collapsed) revealed an FEV1~ 800cc.
What would you suggest as the next step?
Follow-up to drop in ETCO2
Good comments on this case. A drop in ETCO2 suggests a massive mismatch or loss of pulmonary vascular perfusion. Cardiac arrest would do that but I did not describe full arrest. DKeena mentioned esophageal intubation. It can be tricky especially in emergencies when a lot or air is bagged into the stomach and an initially +ETCO2 drops as the tube stays in the esophagus. Massive PE will cause a decrease in CO2-rich blood flow to the lungs. Since her ETT was properly placed and her EKG showed no ischemic changes (just the LAFB) and she is a sedentary (having back surgery, remmember?) I was concerned she had had a PE and requested and emergent CT. Check it out below:
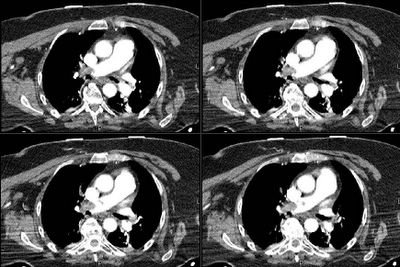
 Would you thrombolyze her?
Would you thrombolyze her?
What would you do next?

What would you do next?
Tuesday, November 01, 2005
Quick follow-up to Asthma (with Strongyloides)
This is the 20 y/o woman with bronchospasm and cough after her missionary trips. She has finished her course of Albendazole and has been on Asmanex (mometasone). She is now assymptomatic, her lungs are completely clear and her FEV1 increased from 2.29L(76%) to 3.30L(110%) and her ratio increased from 80% to 87%. We are weaning her Asmanex off and her repeat stool O&P were negative.
Pancytopenia, abnormal cxr
I hope to have a lively debate because there is some controversy about the following case:
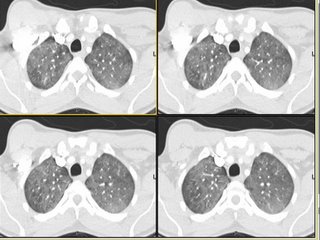
34 y/o AA woman with pancytopenia 10 years ago. Asymptomatic, lost to f/u because of insurance. Refused BM biopsy. 5 years ago gradual onset of dyspnea. May of this year presented with SOB and admitted. (Pulmonary consult called at that time). On exam she had some JVD, clear lungs, loud O2, hepatosplenomegaly, ascites and 2+ pitting edema. Echo showed PAP of 48 with dilated RV and an LV with an EF of 65%. Labs: WBS 2.2 with 82% N, Hgb 9, plts 104. ACE was 207.
CXR and CT:


Bronch BAL not sent, therefore cell count and micro of the fluid unknown. A TBBX showed of the RNL showed a single poorly formed granuloma. The micro on the biopsy *was* sent and was negative. Endobronchial biopsy showed active chronic inflammation.
Urinary histo Ag never sent. Serum Ab's against fungus also not sent.
Questions:
1. Would you consider the above info sufficient stop at the diagnosis of sarcoid?
2. Would you be satisfied with no infectious cause based on negative Tbbx micro, but BAL not sent?
3. Do you feel that a cell count with CD4 and CD8 would have been helpful to you?
4. (corollary to 1): Is there anything else on your differential list besides sarcoid? The person presenting this case to me has no other diagnoses on his list.
5. Does the history of 10 years of pancytopenia rule out histoplasmosis or other fungus?
34 y/o AA woman with pancytopenia 10 years ago. Asymptomatic, lost to f/u because of insurance. Refused BM biopsy. 5 years ago gradual onset of dyspnea. May of this year presented with SOB and admitted. (Pulmonary consult called at that time). On exam she had some JVD, clear lungs, loud O2, hepatosplenomegaly, ascites and 2+ pitting edema. Echo showed PAP of 48 with dilated RV and an LV with an EF of 65%. Labs: WBS 2.2 with 82% N, Hgb 9, plts 104. ACE was 207.
CXR and CT:




Bronch BAL not sent, therefore cell count and micro of the fluid unknown. A TBBX showed of the RNL showed a single poorly formed granuloma. The micro on the biopsy *was* sent and was negative. Endobronchial biopsy showed active chronic inflammation.
Urinary histo Ag never sent. Serum Ab's against fungus also not sent.
Questions:
1. Would you consider the above info sufficient stop at the diagnosis of sarcoid?
2. Would you be satisfied with no infectious cause based on negative Tbbx micro, but BAL not sent?
3. Do you feel that a cell count with CD4 and CD8 would have been helpful to you?
4. (corollary to 1): Is there anything else on your differential list besides sarcoid? The person presenting this case to me has no other diagnoses on his list.
5. Does the history of 10 years of pancytopenia rule out histoplasmosis or other fungus?
Subscribe to:
Posts (Atom)