
Showing posts with label Radiology. Show all posts
Showing posts with label Radiology. Show all posts
Wednesday, February 20, 2008
What's your line?
A resident put in a left subclavian line and maybe went a little too far. An xray shows that it went into the right atrium and into the IVC and up to the IVC filter. When it was removed (with help from vascular), the filter had migrated up 2 vertebrae... Click image to enlarge. It is a bit dark.

Wednesday, December 19, 2007
41 year old with HIV and fever
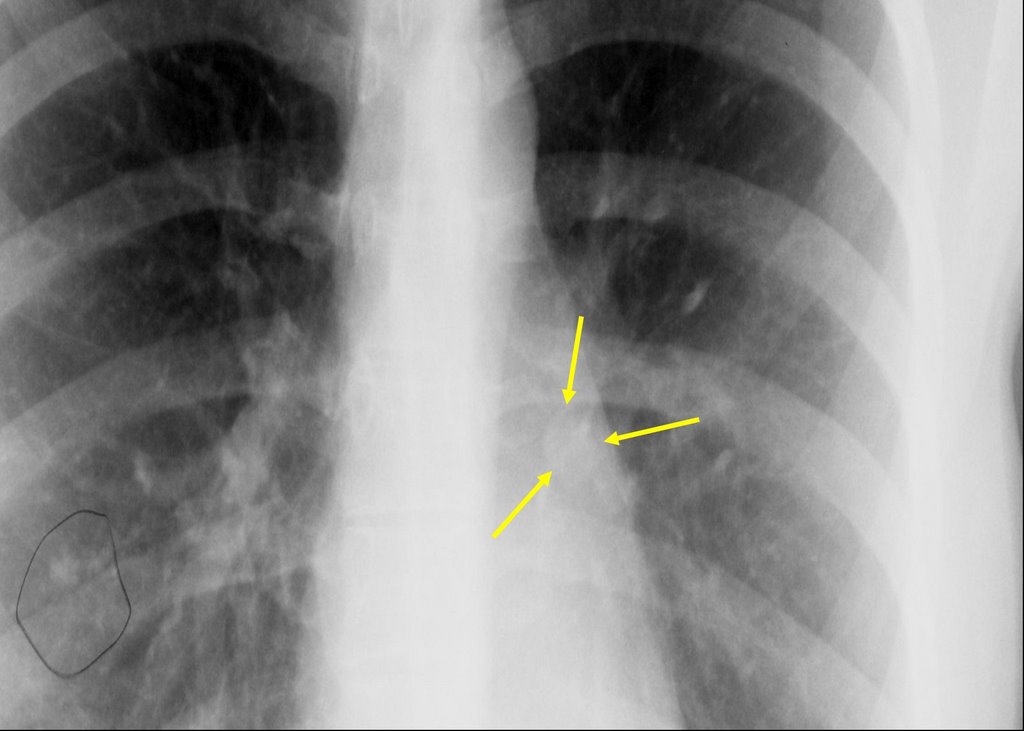
This is a 41 year old man with AIDS, CD4 below 10, who presented with shortness of breath and fever. He was admitted to a general ward but trasnferred to the unit a few days later for tachypnea. On the general floor, his vitals were normal except for some tachycardia. He was 97% on 2 l NC. CXR:

a full workup was done to look for infectious source.
sputums: AFB negative x 3, fungal negative. PCP negative (no PCR, no bacteria
CSF - negative for infection.
What kinds of things could be causing these findings and what would you do?

a full workup was done to look for infectious source.
sputums: AFB negative x 3, fungal negative. PCP negative (no PCR, no bacteria
CSF - negative for infection.
What kinds of things could be causing these findings and what would you do?
Wednesday, September 05, 2007
Pulmonary infiltrates



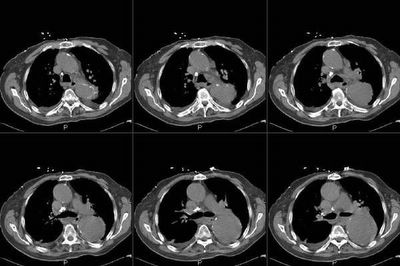
This is a 77-year-old woman who presented with significant cough, dyspnea and hypoxemia and was found to have pulmonary infiltrates. She has been started on aggressive good antibiotic therapy, but continued to have an elevated white blood cell count, dyspnea and cough so we were consulted. No previous label of COPD; never smoked; no heart disease; no odd exposures.
She had not been able to produce significant amounts of sputum. She was also found to be hyponatremic with significant fluctuation of her sodium during her initial hospital stay. Urine and serum Osms were consistent with some SIADH and she improved with fluid restriction. Unremarkable U/A and normal renal function.
She then developed some respiratory distress, mild hemoptysis, worsening hypoxemia and had to be intubated and had the changes seen on the second CxR. (Some cuts from the CT from that day are included).
What would you want to know/do next?
Friday, April 13, 2007
Cavitary mass
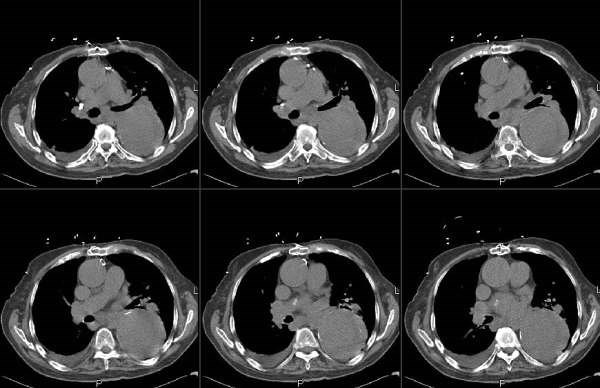
86 year old man with history of dementia brought by his caretaker for mental status changes and lethargy. He lives in an assisted living facility, but has no TB risk factors otherwise (He has his own apartment-like structure, but I beleive there is a common area).
His CT:


There was no hilar or mediastinal adenopathy.
The thickest wall area on that lesion was 4-5 mm.
Someone placed a PPD and it was 11 mm. It was reportedly negative 6 months ago.
He is not productive of sputum, so 3 gastric lavages were done and they were all negative. What would you do next? Are you worried about active tb? Here are my thoughts
1. How sensitive is gastric lavage for afb?
2. location of the cavitary mass is not where tb should be.
3. is he a ppd converter, or was he anergic or are we seeing a booster effect
4. His family does not want an aggressive w/u for cancer, but on the other hand one would not want to send someone home to hospice with active tb....
His CT:


There was no hilar or mediastinal adenopathy.
The thickest wall area on that lesion was 4-5 mm.
Someone placed a PPD and it was 11 mm. It was reportedly negative 6 months ago.
He is not productive of sputum, so 3 gastric lavages were done and they were all negative. What would you do next? Are you worried about active tb? Here are my thoughts
1. How sensitive is gastric lavage for afb?
2. location of the cavitary mass is not where tb should be.
3. is he a ppd converter, or was he anergic or are we seeing a booster effect
4. His family does not want an aggressive w/u for cancer, but on the other hand one would not want to send someone home to hospice with active tb....
Tuesday, March 27, 2007
Where is Waldo (or the line)?



As ICU co-directors we get to see some unusual situations. This line was reportedly a "little traumatic" going in and there is no good blood return from any of the ports. I enlarged the segment of interest and crudely followed the trajectory. Where is the line going?
Friday, February 23, 2007
Digging for gold




This nice woman with mild asthma lost a tooth crown and aspirated it as she was about to have lunch.
Check out the CxR. It was lodged at the first branching of the R bronchus intermedius with the smooth side (the shiny top of the crown) up towards us. Unfortunately I was using an optic (as opposed to digital, I know they are all "optic") scope and couldn't take a picture. I did snap a picture of the crown after removal with the basket on the side.
We did not have a bronch basket handy so an OR gallstone basket was just the perfect sixe.
Friday, September 15, 2006

Thursday, August 03, 2006
Halleliujah
From Arenberg:
"In celebration of the fact that the IT people in the Department of Radiology at the University of of Michigan have recognozed that their department exists to provide films for other doctors to look at, and have finally made it into the 21st centry by providing consistent, relaible online access to films for the unwashed masses (read: non-radiologists)...I hereby submit this film of an unfortunate man with a history of cancer."

"In celebration of the fact that the IT people in the Department of Radiology at the University of of Michigan have recognozed that their department exists to provide films for other doctors to look at, and have finally made it into the 21st centry by providing consistent, relaible online access to films for the unwashed masses (read: non-radiologists)...I hereby submit this film of an unfortunate man with a history of cancer."

Monday, June 19, 2006
Radiology monday
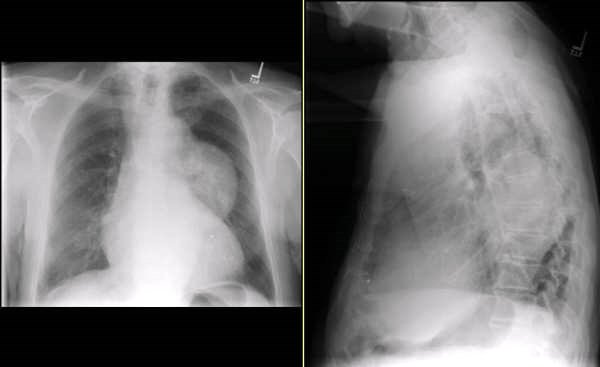
This 72 year old man is asymptomatic and had a routine chest xray as part of a yearly exam from his primary care physician.


Tuesday, June 13, 2006
Follow-up to Radiology Thursday
Jennings picked up on the Left mediastinal mass. The patient could not stand up for the lateral so a CT was obtained:


Thursday, June 08, 2006

Tuesday, April 11, 2006
collapsed RML
Check out Jeff's post below.

I hate to answer a question with another question, Jeff but I have had this similar case. This is a 65 y/o woman, no significant TOB Hx with recurrent partial LLL collapse. She has had LLL CAP 3 times (see above) and though the pneumonias clinically all resolve (they have been over ~ 5years) she always has a residual partial LLL collapse. She was bronch'ed in 2001, 2002 and I have re-bronch'ed her in 2005. Her airway though a little narow with some dynamic collapse looks normal and biopsies and Cxs were also all negative.
Other than encouraging pulmonary clearance, chest P&PD, etc. would you do anything else?

I hate to answer a question with another question, Jeff but I have had this similar case. This is a 65 y/o woman, no significant TOB Hx with recurrent partial LLL collapse. She has had LLL CAP 3 times (see above) and though the pneumonias clinically all resolve (they have been over ~ 5years) she always has a residual partial LLL collapse. She was bronch'ed in 2001, 2002 and I have re-bronch'ed her in 2005. Her airway though a little narow with some dynamic collapse looks normal and biopsies and Cxs were also all negative.
Other than encouraging pulmonary clearance, chest P&PD, etc. would you do anything else?
Friday, April 07, 2006
Radiology Friday. 20 year old female

Friday, March 10, 2006

{kind=link}
{kind=link}
{kind=link}
Wednesday, February 15, 2006
Follow-up to Wednesday Radiology - Case 2
'Can't hide anything from these smart people.
Check out the CT (unenhanced because Creat is 2.0). We did not feel like biopsying the "mass" either...
Check out the CT (unenhanced because Creat is 2.0). We did not feel like biopsying the "mass" either...

Radiology Wednesday - Case 2
We were called by one of the cardiologist for this abnormal CxR. How would you approach the radiographic abnormality?
Radiology Wednesday
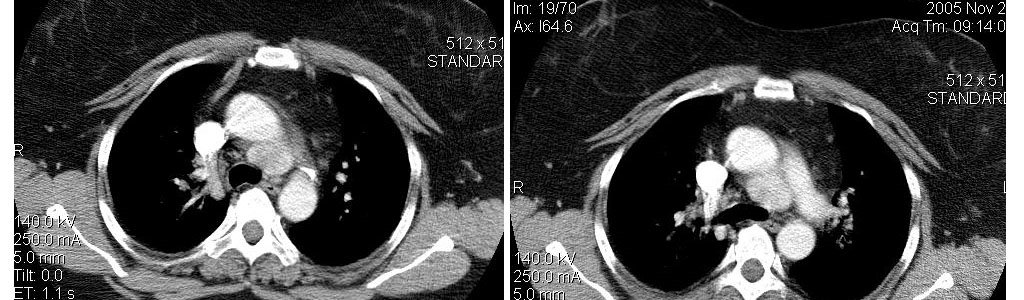
This was submitted by D Arenberg:
This is a contrast chest CT. What's the differential diagnosis?

This is a contrast chest CT. What's the differential diagnosis?
Subscribe to:
Posts (Atom)