43 year old presented with 6 weeks of progressive dyspnea associated with URI-type symptoms. Had recieved several courses of antibiotics as an outpatient. No fever/chills. + non-productive cough. No associated s/s. Non-smoker. No occupational exposure. On presentation, he was hypotensive, but alert and oriented. His was quite comfortatble despite profound hypoxia (initial oxygen saturation of 62% on room air). Physical exam has some scattered rales. WBC is 4, without a shift. Blood count and platelets are normal. He is hypoxic, requiring up to 100% supplemental oxygen by non-rebreather to maintain a pO2 in the 60's. His ventilation is adequate, with a pCO2 of 42 and a pH of 7.39.
A CT scan shows:

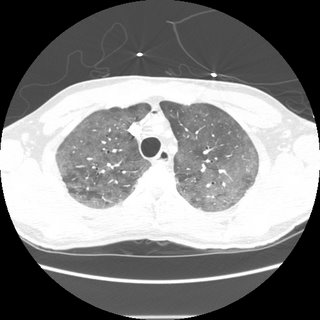


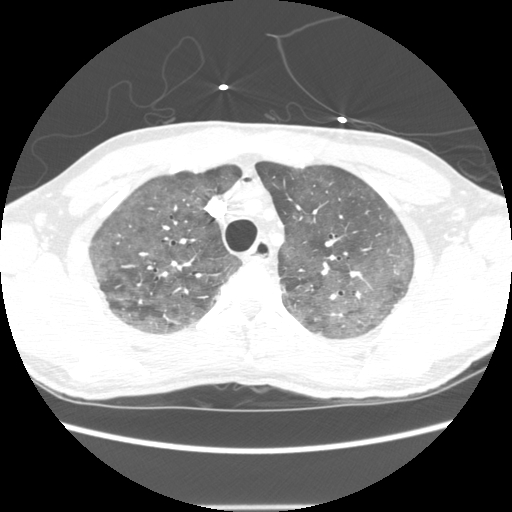

4 comments - CLICK HERE to read & add your own!:
well, progressing hypoxemic respiratory failure in a non-smoker. No response to antibiotics. The ddx depends on some things in history. What's his age and immune status? If HIV, would consider PCP. If not immunosuppressed wou;d consider eosinophilic pneumonia (don't know time course of his dyspnea but would likely be the chroniuc eos pneumonia). Acutre phase of hypersensitivity pneumonitis given the right exposure history.
If he has an underlying collagen vascular disease lupus pneumonitis might be considered. Non-smoker makes DIP and RB-ILD less likely.
In the right clinical context I suppose PAP would be a consideration.
Then there is the idiopathics such as NSIP and even LIP.
Of course there is also bronchoalveolar carcinoma.
W/u (after more detailed history, if pertient), would be a BAL and tbbx to workup all the things outlined above.
The remainder of his history is really non-contributory. His HIV-status is not known. He initially refused bronchoscopy.
Empiric therapy?
More like a shotgun followed by a two by four and sledgehammer chaser.
Patient got steroids and most antibiotics known to mankind. He eventually agreed to bronchoscopy. I'll finish this up tomorrow, in case anyone else wants to throw in their thoughts.
Going...going....gone:
So, it turns out the patient refused an HIV test, which is probably the strongest indication out there of his diagnosis.
He had a bronch with BAL, and developed a pneumothorax ON THE CONTRALATERAL SIDE TO WHERE ALL SAMPLES WERE TAKEN.
The pulmonary pathologist called with the diagnosis before the sample was even processed or looked at under the microscope.
Diagnosis:
1) PCP
2) Aids
3) Pneumothorax (iatrogenic?)
Jennings hit it out of the park in line 1. Clinically, he was started on Bactrim the morning after he presented, but before any other testing was obtained. He's still critically ill, after 1 week of appropriate therapy.
Post a Commenttest post a comment