This is a 43 y/o man with previous Hx of mild HTN. He had been told before he had a "big heart" but had no further specific w/up.
He came to see us with a dry cough, dyspnea on exertion (progressive) and orthopnea. No PND, no lower ext. edema.
His HTN has been worse and he is requiring 4 anti-HTN meds. He has been found to be "borderline diabetic" and a CxR showed again a "big heart" with large RV.
His exam revealed central exp. wheezing and elevated BP.
His spiro revealed moderate obstruction.
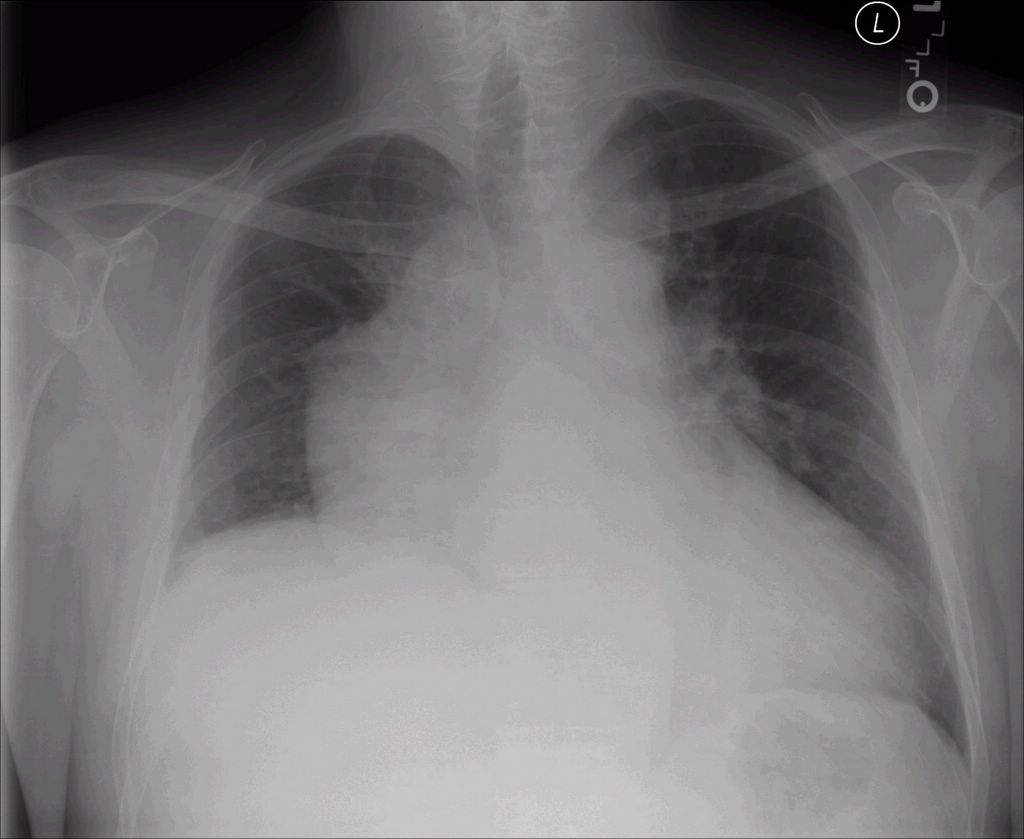
Here is his PA with the "big heart"
And lateral...

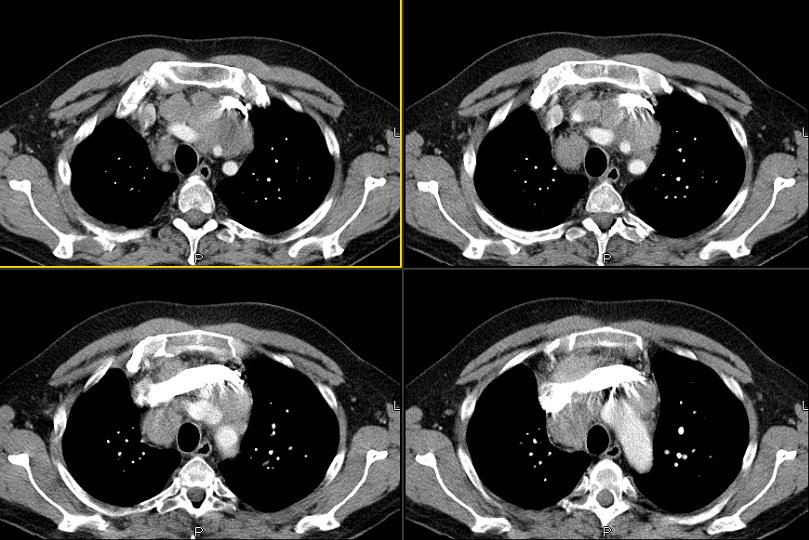
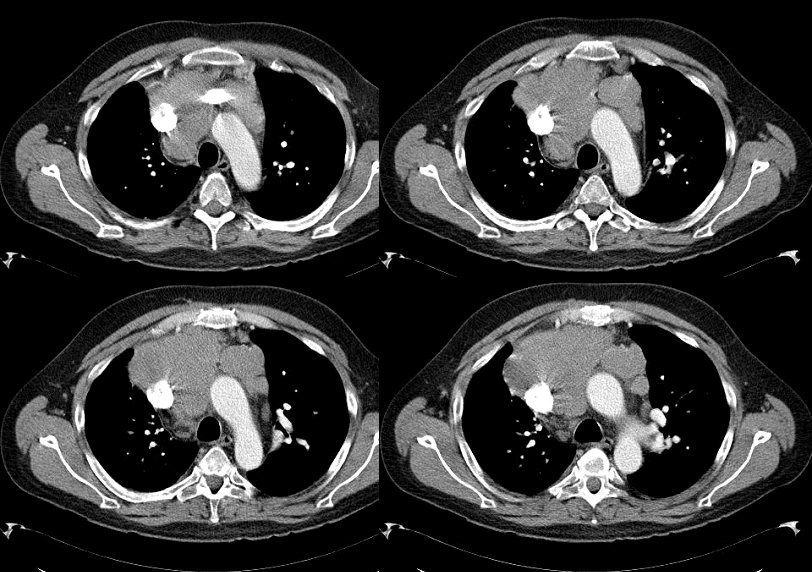
Here are some representative slices from the CT:

Differential Diagnosis?
BTW, he doesn't smoke. Any suggestions? (JJ, you know the case so don't give it away).
BTW, he doesn't smoke. Any suggestions? (JJ, you know the case so don't give it away).
10 comments - CLICK HERE to read & add your own!:
I combined all into one post - hope you dont mind.
That's pretty impressive. Just on the PA and lateral, I would have said he's got a huge RA and RV. But on the CT scan, this looks like an anterior/superior mediastinal mass encasing the left subclavian v. Additionally, the pulmonary outflow tract looks very prominant, and while it may just be the cuts you've shown, I don't see the left pulm. artery. It's hard to tell if they are separate from the mass, but there may be some pre-vascular LAD as well.
Although I don't see any calcifications, if this has been long-standing and not progressive I'd think about fibrosing mediastinitis. Of course, sarcoma/lymphoma/thyroid carcinoma are also possible. I think he needs a biopsy--? mediasteinoscopy vs. an open surgical biopsy.
By the way---this thing amazingly looks a lot like a liver sitting in his thorax!
HTN requiring 4 meds....
Location is very atypical for a pheochromocytoma, but I guess that's a possibility. Or am I missing the elephant in the middle of the room?
No you're doing fine baw.
wheezing..HTN
He had a bronch which showed no endoB lesions and we sent him to see the CT surgeons. I'll give out more details after Lazar and Mendez had a chance to take a look. The mass is really very impressive. The PA was not occluded on the other cuts but the SVC was starting to get a little tight (though clinically he has no SVC synd).
Mike M brought up a good point on the carotid. On upper cuts it did not occlude the carotids. We had the same differentialwith the four T's. He underwent surgery and that whole thing (>20cm on long axis) was a carcinoid!
He did not have carcinoid syndrome but his HTN, glucose intolerance and weakness were due to Cushing's: his ACTH was high with a cortisol ~70, consistent with an ACTH-producing mediastinal (possibly thymic) carcinoid.
Fascinating case. I did not have a chance to view the blog over the weekend (Comcast is "updating" in the WB area).
How certain are they that it is carcinoid and not a Neuroendocrine tumor that is secreting ACTH (i.e. small cell)?
This was a very well differentiated carcinoid with very typical architecture. There is some data for thoracic carcinoids secreting ACTH and the controversy is whether they are more aggressive than bronchogenic tumors or not.
http://www.sciencedirect.com/science?_ob=ArticleURL&_udi=B6T11-4FSTRWK-B&_coverDate=04%2F30%2F2005&_alid=277663881&_rdoc=1&_fmt=&_orig=search&_qd=1&_cdi=4877&_sort=d&view=c&_acct=C000050221&_version=1&_urlVersion=0&_userid=10&md5=b129a07701d1c9b1b3fe41d7e0fbe2d1
Post a Commenttest post a comment