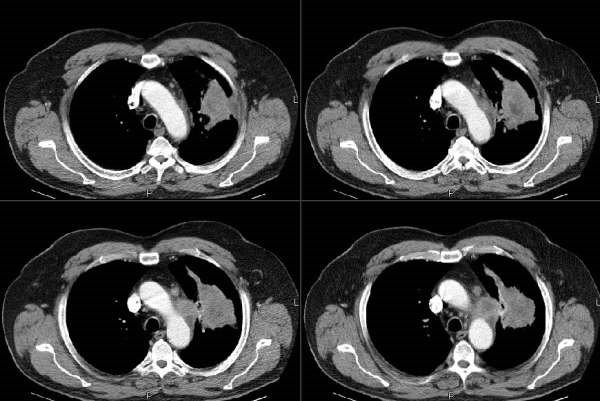
This is a man in his 60's with no previous lung or heart disease. He presented to the ER with atypical R-sided CP, had an abnormal CxR and had the following CT:
I saw him in our office, he has an occasional cough and normal PFTs.
I did a bronch which showed no endobronchial lesions but confirmed a NSCLCa (squamous).
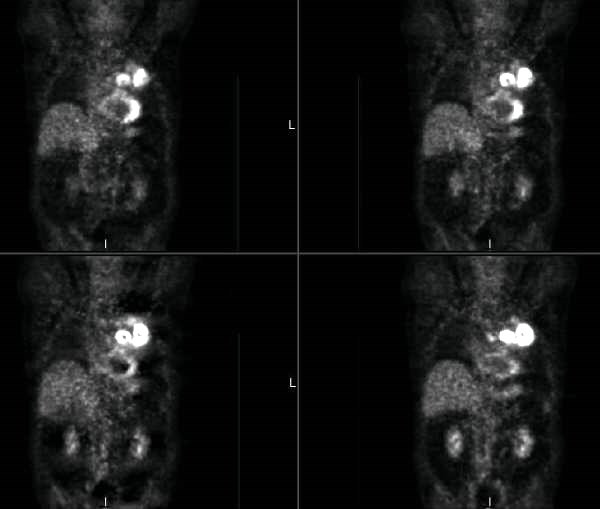
His PET scan showed obvious uptake by the mass and an ipsilateral node.
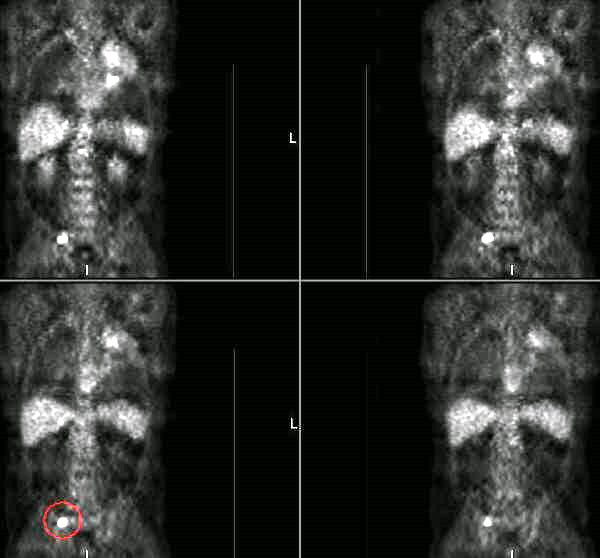
It also showed some increased uptake in the sacrum:
The sacral area is anterior and not approachable by CT-guided Bx... What would you do next? With the PET but no tissue confirmation from the sacrum would you consider him a stage IV? Would you try and get a surgical Bx from the sacrum?
7 comments - CLICK HERE to read & add your own!:
There are several questions that I have about the case.
First, how did you get the diagnosis on bronch? Washing? Brush? Wang?
If everything is as billed, he has a Stage IIB lesion (assuming the sacrum is negative) and should be offered a curative surgery.
If the sacrum is positive, he has stage IV disease and would be a chemo/xrt candidate.
So, he needs a biopsy of that lesion.
By the way, why did he have the atpical Right sided pain? Is there something I am missing on my miserable monitor?
The Dx was confirmed on TBBx and BAL of the upper lobe lesion. There was no splaying of carinas and a a hilar FNA was negative.
The CP was kind of a red herring, more like an URI that resolved fast...
I agree with the need to address the sacral lesion. The problem is the access... he will need an ortho surgical biopsy from an anterior access.
I think that, ultimately a biopsy of the sacral lesion is necessary. First, however, I would do further imaging (CT or MRI of the sacrum), as bony metastases can have a "classic" appearence on CT.
Ipsilateral node looks mediastinal. You are likely dealing with clinical N2 disease( at least stage 3A). CP is suspicious for bone mets. I would get a bone scan and an MRI of the head (esp. if it is adeno) together with CT of the abdomen and pelvis before considering surgery.
Oops, I did it again. It is squamous. I still consider an MRI head. I did not read carefully enough.
I suppose I should have looked closer at the CT before staging the lesion... my apologies for the IIB comment.
Some institutions still operate on IIIA lesions, but I am not sure of the data. Any role for neoadjuvant chemo/xrt and then restaging?
Arenberg, I guess you are right. A bone scan is not necessary unless you are suspecting bone mets from osteosarcoma. And it is very unlikely in this case.
Post a Commenttest post a comment