really had any cough. Denies any fever, chills, rigors, chest pain, or weight loss. Denies any hemoptysis. Denies any previous infections. Denies any headache, nausea, vomiting, or diarrhea.
AST MEDICAL HISTORY: Peripheral vascular disease, hypertension, hyperlipidemia, previous history of smoking.
MEDICATIONS: Atenolol, Protonix, Procardia, hydrochlorothiazide, Lipitor, TriCor, aspirin, multivitamins, and Tylenol 3.
SOCIAL HISTORY: 50-pack-year smoking history, stopped 2 years ago. No ETOH or drug.
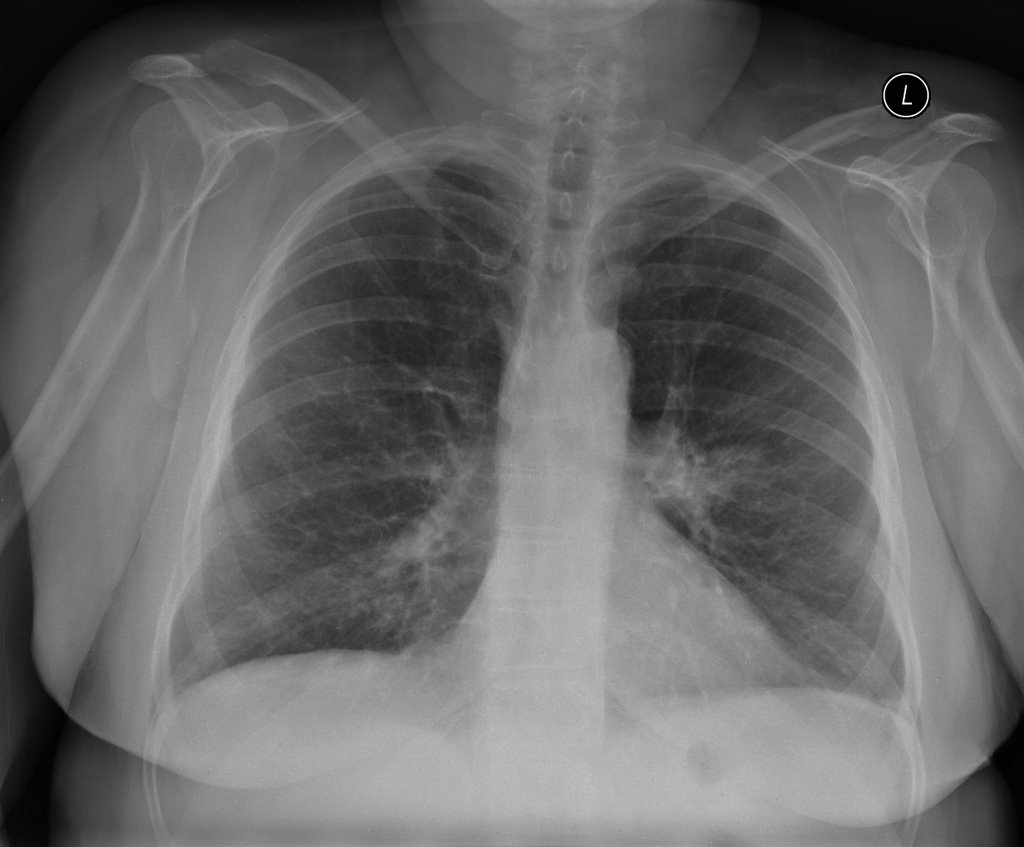
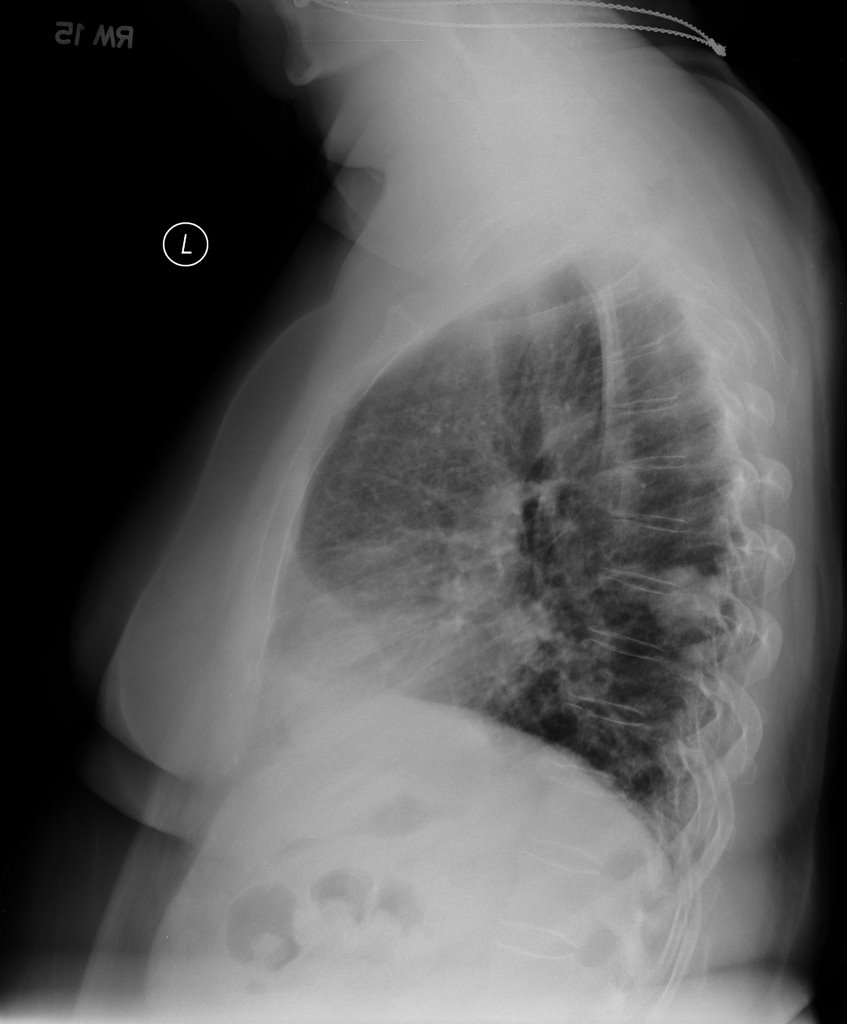
No mediastinal or hilar adenopathy.
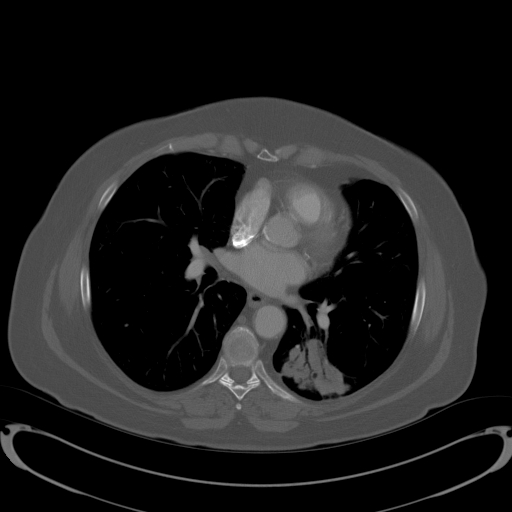
Repeat CT 1 month later showed no change in size.
Patient was bronched with non-diagnostic tissue.
Cytology brush from left lower lobe was negative for malignant cells.
Micro on BAL: 30000 CFU per ml alpha-hemolytic Streptococcus, 8000 CFU Neisseria; 9000 CFU Micrococcus; 5000 CFU Streptococcus, non-hemolytic.
What would be your next step (or any other questions you have)?
1 comments - CLICK HERE to read & add your own!:
The one CT cut makes it look like air-space dz (with air bronchograms and all) but in someone with that much TOB history I would still be very suspicious for a malignancy (BAC could look like that).
You have mentioned no interval change in the CT. Did she get ABTx between scans.
The BAL flora looks like oral flora. It is a funny picture and presentation for aspirtaion...
I see a couple options: give ABT xand repeat the CT in another month (only two months from initial scan); repeat bronch after ABTx or ask radiology to try and aspirate some of that area for Dx.
Post a Commenttest post a comment