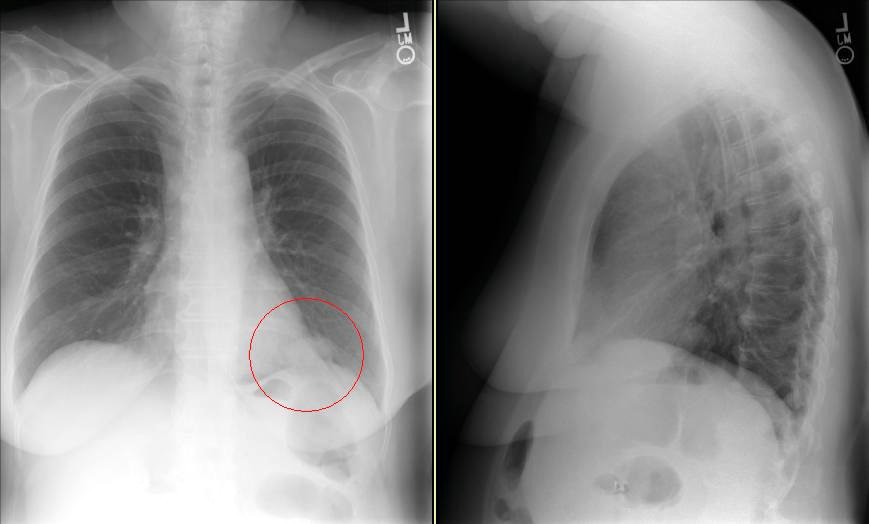
This patient came to me pre-worked up so I will show all the data she had had thus far. This is a 65 y/o woman with no TOB Hx, normal PFTs who had a persistent cough. She had an abnormal CxR (see above) and here PCP ordered a CT and then a PET-CT and she was sent to us.
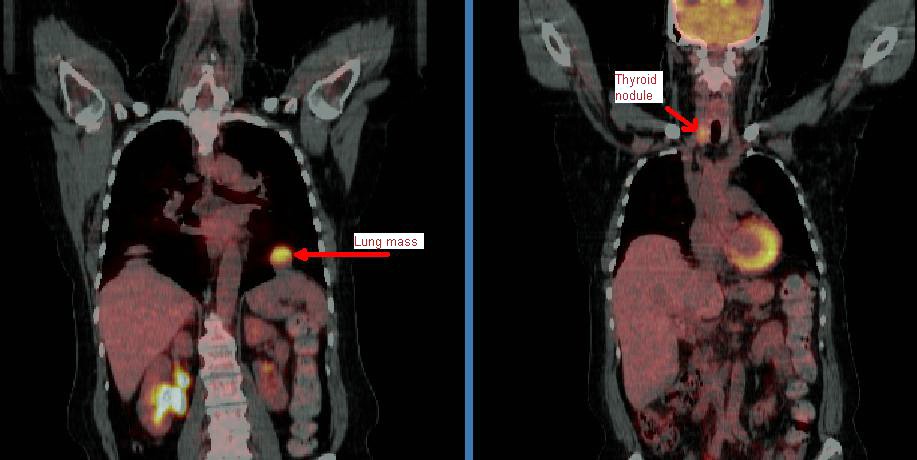
Her PET scan showed two very FDG-avid lesions. A L basilar lung lesion and a R thyroid nodule with no other abnormal uptake. She is euthyroid clinically and by TFTs.
Do you think the lesion are related?
Would you biopsy one, the other, both?
2 comments - CLICK HERE to read & add your own!:
I had a very similar consult recently, except the patient had severe COPD (FEV1 0.7) and a large nodule abutting the chest wall. I recommended starting with a biopsy of the thyroid to avoid the risk of a PTX. Path came back suggestive of papillary ca, but they couldn't call it. Ended up biopsing the nodule, after which the stains suggested the thyroid was a metastatic lesion from the lung primary (mucinous adeno).
I think anaplastic thryoid ca's are the most likely to spread to the lung, but I've heard the thyroid lesions should be pretty large by that point.
Cool case: What does the thyroid lesion look like on the transmission CT images? A recent Journal of Nuc Med article looked at this: If the lseion appears primarily cystic, it is very unlikely to be cancer.
Probably best to bx the Thyroid first otherwise. This case could easily represent 2 sepearate primaries.
Post a Commenttest post a comment