He was started on steroids and plaquenil (the latter by his PCP/rheumatologist) with good resolution of his constitutional symptoms. He was weaned off the steroids over a 6 month stretch. The wean finished about 2 weeks ago.
Initial CT scan in August (conventional CT)

Was seen about 1 week ago after completely weaned off prednisone. Has been having some increased dyspnea over the last 1-2 weeks that is somewhat related to exertion, but not completely.
PFT's: Normal spiro and lung volumes. DLCO ~61% predicted. DLCO in November was ~72% predicted.
Repeat CT chest (this time with HRCT protocol).
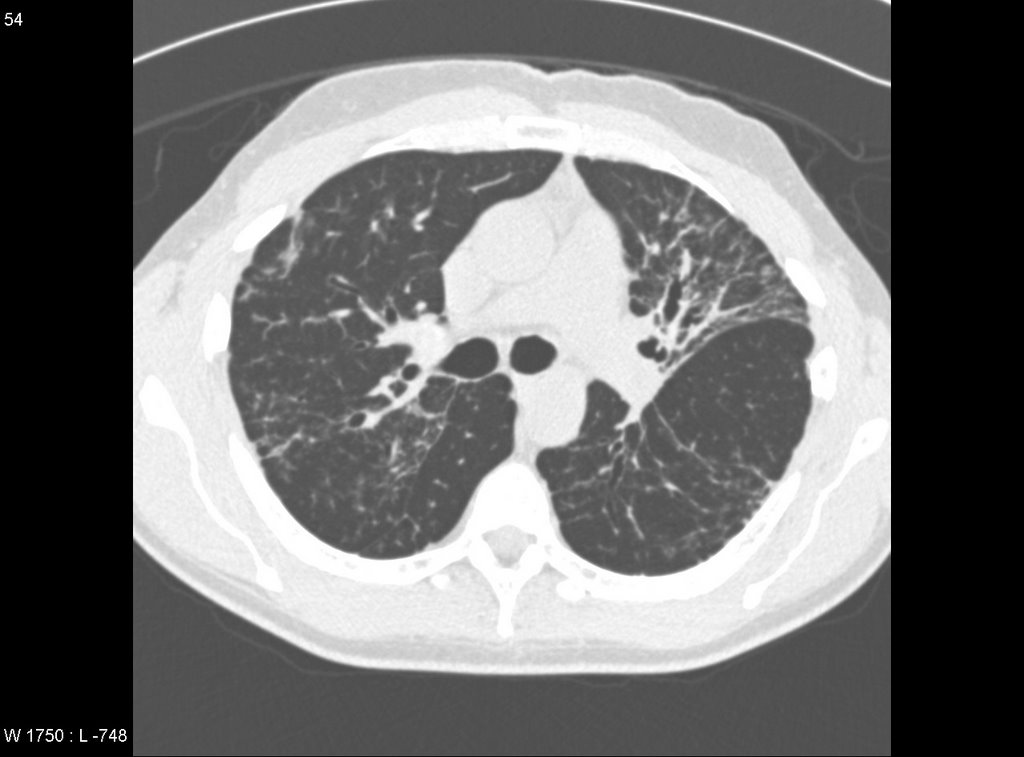
The majority of the lung is actually normal. There are a few cuts with the above parenchymal abnormalities.
What would you do?
4 comments - CLICK HERE to read & add your own!:
Let me re-cap before a comment to make sure I understand:
He had dyspnea and constitut sx that improved on steroids. The steroids are off for 2 weeks and he develops increased dyspnea. A f/u spiro shows a DLCO of 61%, down from 72%. An HRCT shows improvement.
Is that correct? Where was he in terms of steroids when the 72% was done? Does the 61% represent a time when he was off steroids? Is the HRCT off steroids? Was he SOB when that HRCT was taken?
I guess one of the questions here is whether he is dyspneic because of the sarcoid despite radiographic improvement or is there a second reason?
His DLCO has decreased even though the lungs look better. It seems the primary Dx of sarcoid is pretty solid with Bxs to seal it.
I might consider looking for other reasons for the change (ECHO, bubble study looking for shunt, TSH, maybe a V/Q, etc.). If there are no obvious cardiac or pulmonary-vascular changes I would probably try a CPET to help identify the source of dyspnea as he may even have a steroid myopathy.
Jennings recap is accurate.
Nice thoughts.
I did not work him up for a PE as he is pretty active and no recent traumatic injury. His original CT in august was with PE protocol and was negative.
His TSH is normal.
Any other thoughts? Would you still get a V/Q?
After steroids were stopped his DLCO went from 70% to 62% (but with an HRCT showing radiographic improvement). But a DLCO is still more sensitive for detecting early diffusion abnormalities than HRCT, so if you have ruled out other causes, I would either restart the steroids or consider a steroid-soaring agent at this point.
Other causes to rule out were as Baleeiro and Arenberg stated, namely echo with bubble and maybe a PE-CT: I am sure a V/Q would liklely come back as intermediated and then you'd be stuck.
Post a Commenttest post a comment