38 year old white female with PMH of interstial cystitis presented to ER by EMS after she was found to have a seizure at home witnessed by her mother. That was her second seizure and her initial one was 1 month ago when she went to an outside local hospital. Her work up at that time included head CT which was negative except for sinus disease. She was advised to follow up with her PCP at that time.
In the emergency room, she was afebrile but post-ictal. She was also hypoxic. She was put on oxygen and admitted.
PmHx only significant for the interestitial cystitis. Had some ankle edema 6 years ago treated with low salt diet; thought secondary to her job standing all day (dishwasher).
Medications: none.
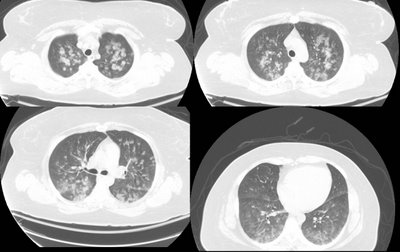
CT scan:
RF and sed rate low or normal.
What are your thoughts and what would you do?

2 comments - CLICK HERE to read & add your own!:
That's a funny CT for aspiration. I guess since she was seizing she may have been in an awkward position and developed some upper aspiration pneumonia... It is also not typical for nitrofurantoin-related ILD if they are giving it to her for her cystitis. Even post-seizure (neurogenic) edema would not fit well with the CT...
It looks more like an alveolar pattern, maybe just regular CAP and it lowered her seizure threshold.
The transbronchial biopsy showed "Rare intraparenchymal crystalline material, otherwise unremarkable lung parenchyma" The BAL cell count and diff was unremarkable, with about 75% macrophages. All micro studies were negative as well. Serum ANA and RF were negative. The sed rate was 15.
The EEG showed interictal expression of localization-related epilepsy and MRI showed non specific hyperintensity within the left frontal lobe. Neuro consult recommended Lamictol.
Any other thoughts?
Post a Commenttest post a comment