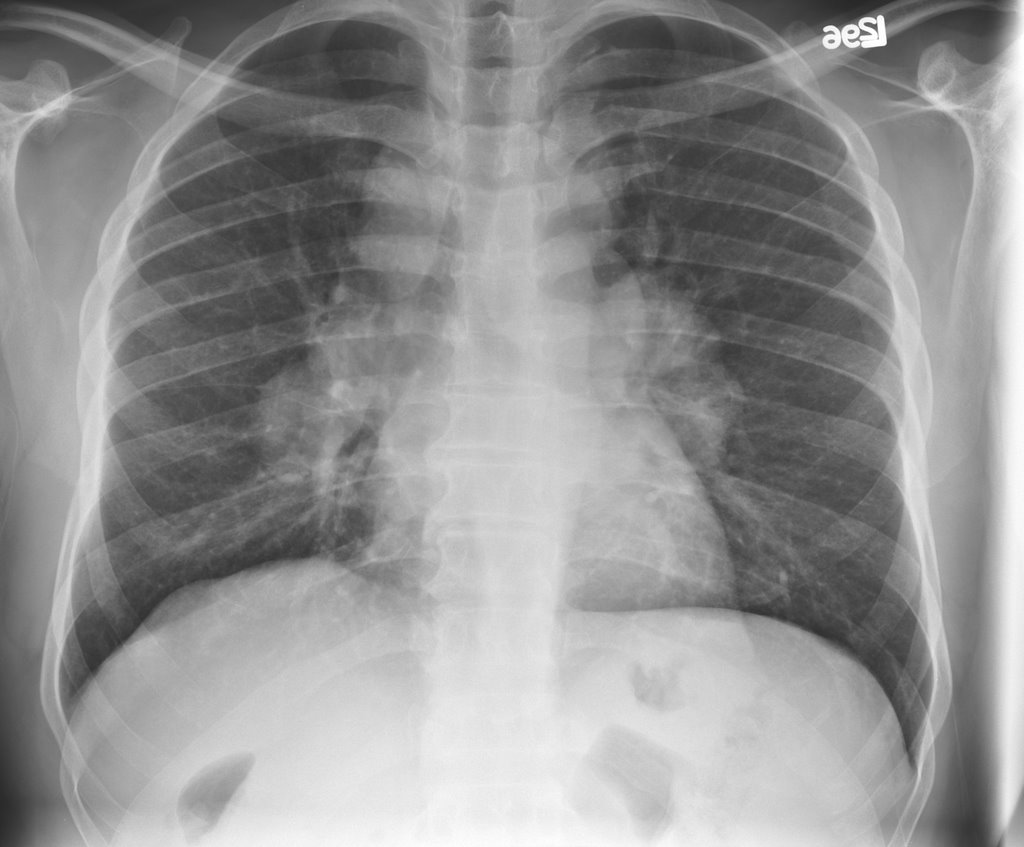
His PFT's were normal. LFT's were slightly elevated (Alk phos 192, GGT 152) with a normal ultrasound and no abdominal complaints. A presumptive diagnosis of sarcoidosis was made and the patient was simply followed. 5 months later he c/o subjective fever and night sweats. No respiratory symptoms. A chest xray was actually improved:

What would you do? Are you still satisfied with the diagnosis of sarcoid? (I am aware of a study that found that in almost all cases with symmetric adenopathy, the dx is sarcoid.) WOuld you want to definitely dx it or rule out other causes?
If you are satisfied with the dx, how would you handle the constitutional symptoms? Assuming f/u PFT's are not in decline, would you treat these B symptoms with immunosuppressive therapy?
12 comments - CLICK HERE to read & add your own!:
I would be concerned with the new symptoms. A few questions: is he a smoker? Was a CT scan done on his first presentation?
I would consider ruling out infectious etiologies (or even a lymphoma) before starting him on immunosuppression.
I guess my concern is not so much whether the initial Dx was correct but whether he now has a superimposed process.
Well, the adenopathy is decreased on follow-up cxr. Also, the hilar adenopathy was pretty classic for sarcoid so a CT was not thought to be necessary.
I agree completely with the initial management. However, now the clinical situation has changed, and we need to ask a few questions:
-Given the regression of the lymph nodes, are the current symptoms related to the previous finding of hilar lymphadenopathy?
-If we think they are related, what is the likelihood that the current symptoms are due to sarcoidosis?
Also, what has happened with the liver enzymes?
Overall, "B" symptoms are not common in sarcoid, and I definitely would not treat without a definitive diagnosis. In fact, even if I had a definitive diagnosis of sarcoid, I would still want to fully evaluate for infectious etiologies (I agree lymphoma is less likely here, but we also can not afford to miss it in this setting) prior to treating for sarcoid.
His LFT's were only mildly elevated and they are now normal except for an alk phos which is 192 but is lower than previously (GGT high to go with alk phos, total bili normal). Previously, hepatitis B antigen negative, hepatitis C antibody negative, HIV negative, RPR negative.
I haven't seen him yet for followup, but looking at other labs, his creatinine is up to 1.6 with his fatigue, so these B symptoms may have nothing to do with the sarcoid after all. In fact, as pointed out in above comments, his adenopathy is decreased.
Renal involvement in sarcoid is VERY rare, but I have seen a case.
You may want to recheck a calcium as this may unify all of the diagnoses (renal insufficiency, sarcoid, B-type symptoms). If not, I would probably start the workup for his creatinine elevations and send him to see a nephrologist.
Ok his calcium came back as 11. With the above info, would you treat? (obviously the calcium level would be treated as well)
I would still look for alternative diagnoses, as hypercalcemia can occur with various paraneoplastic processes. That said, I now think that Sarcoidosis is more likely; but, I think that the obligation here is to evaluate for reasonable alternatives.
I think we are all on the same page that with changes in clinical presentation we would all want to rule out other processes.
His calcium was about 14 when corrected for his albumin. His creatinine was up to 2.0 when I saw him. I admitted him and he was treated with IVF (and steroids for the underlying sarcoidosis that was causing the hypercalcemia). Incidentally, his PTH was <2.0.
I don't think a workup for malignancy is necessary in this patient, as it seems quite apparent that it is due to his sarcoid. Does anyone think otherwise?
How many clinicians are aware of the fact that the use of Accutane in a patient's life (years before diagnosis of sarcoid)predisposes them to sarcoidosis and hilar adenopathy?
I am in the 3rd year of care following a serious case of Valley Fever (Coccidiodes Fungus) contracted in Phoenix AZ in 2004. Several days in hospital followed by 46 IV treatments of Amphotarison B. Long term antifungal medication (Dyflucan/Fluconazole) and they are still trying to figure out why the Lymph nodes in my chest are 4x larger than normal, chronic fatigue and labored breathing.
I come across this preceding statement and nearly fell of my chair. 'How many clinicians are aware of the fact that the use of Accutane in a patient's life (years before diagnosis of sarcoid)predisposes them to sarcoidosis and hilar adenopathy?'
I have 2 bouts of Accutane, one is my youth (1980) and late twenties (1994).
Can this actually be the cause of my adnopothy?
I was on Accutane in the late 80s and was diagnosed with cutaneous, lung, and lymphatic sarcoid around 2001...is there a link?
Post a Commenttest post a comment