No other pertinent family or social Hx.
His exam was remarkable for bibasilar "dry" crackles. No clubbing.
PFTs revealed FVC and FEV1~ 53% with a TLC~ 60% and DLCO also ~65%.
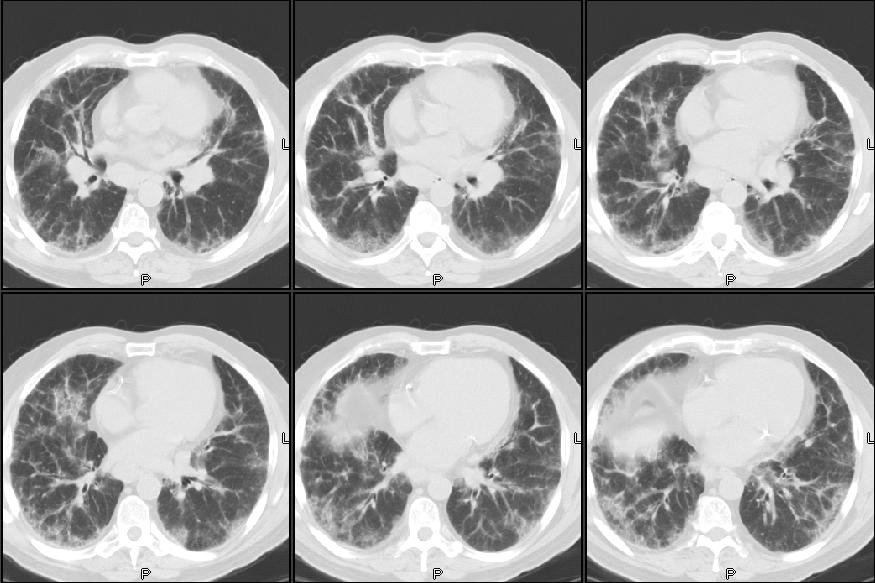
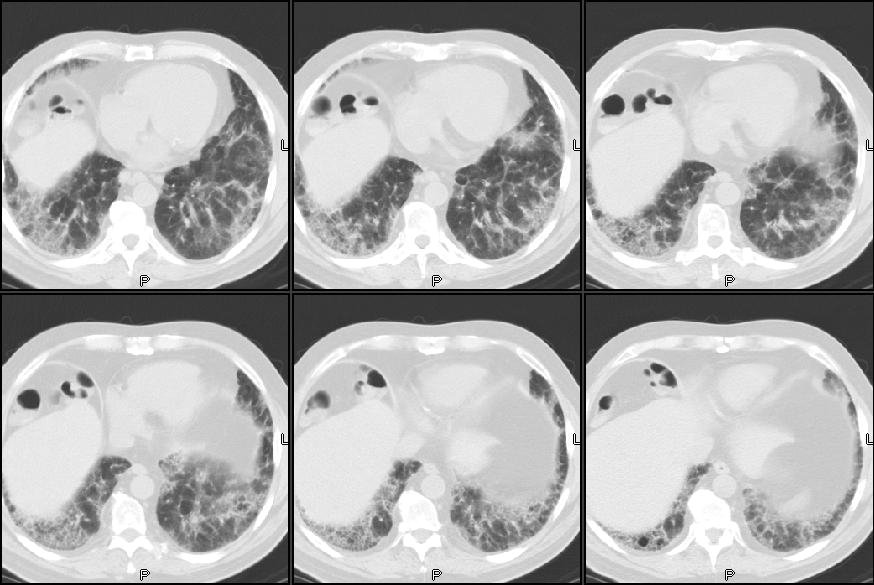
CT scan is as seen below. He had had some lab work prior to seeing us and we ordered some other tests. Of not he had a peripheral eosinophilia (11.2% - 850) and high IgE (670), ESR was 58 and ANA was negative.
A bronch revealed no eosinophils, fairly pauci-cellular BAL, negative Cxs and smears and TBBX showed some interstitial fibrosis, pneumocyte hypertrophy but was basically non-specific.
Would you regard this as "just" IPF or would you make anything out of the Eos and IgE?
3 comments - CLICK HERE to read & add your own!:
Yea, I'm not sure what to make of the peripheral Eos/IgE in this patient. I agree with DA; I would not consider this a "classic" CT scan for UIP. There seems to be quite a bit of ground glass, and although there may be some "honeycombing" toward the bases, I don't think that it's classic.
So, in either case, I think the next step is a surgical lung biosy.
I agree the peripheral eos may not be related, since the BAL was negative for eosinophils. In addition, the CT looks like some ground glass, but how many mm were the slices? I agree NSIP or fibrotic NSIP are possibilities. An open lung would allow you to look for this pattern or to see if there is eosinophilic infiltration, etc.
This seems like a case of PIE syndrome. A complete drug history should be elicited if not done yet. Helminthic infections should be ruled out, depending on the patient's geographic location and travel history. DIP, CVD associated ILD and Hodgkin are also known to be associated with peripheral eosinophils.
Post a Commenttest post a comment