Pleural fluid:
pH = 7.38; Glucose: 43, LDH: 746, Protein 5.0
Gram stain: No
RBC: 496100 WBC: 1000 (< 0.1 N, 52 L, 45 M, 3 E)
Hct 11.3%
Cytology:
- HEMOSIDERIN-LADEN MACROPHAGES IDENTIFIED
- RARE ATYPICAL CELLS, FAVOR REACTIVE MESOTHELIAL CELLS
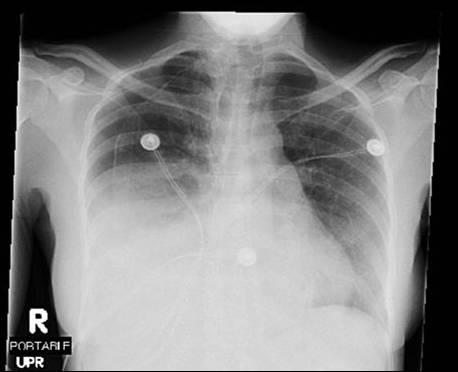
Post procedure CXRs (these are taken 1 day apart, the first being just after the thoracentsis)


Now what?
10 comments - CLICK HERE to read & add your own!:
Well, like I mentioned in first post (later shot down by mendez) could this still be catamenial now that we have all that blood in there? Other causes of this much blood of course brings us back to a malignancy. Still would want an abdominal-pelvic CT to look at the ovaries and for other masses.
Another interesting think would be: does she have ascites and if so is it *also* bloody? That would imply again that the promaryu prob is the abdomin and and the pleural effusion is there from the diaphragmatic holes.
So, what is a "promaryu" problem? (jk).
I agree with the ? about ascites (and asked that in my original post). With the bloody, lymphocytic pleural effusion, I remain suspicious of malignancy and, give the lack of any real change in the CXR post-thoracentesis (how much fluid was taken out), remain suspicious of an abdominal source.
I agree with the ascites issue: if she has a sympathetic effusion because of ascites that would explain the rapidity with which it re-accumulated. Did u check triglycerides in the fluid?
Any abdominal imaging available?
I took out 1.7 liters of fluid.
Triglycerides were not checked, but the fluid appeared bloody.
She was not dyspneic prior to the procedure and this did not change after the procedure.
The cytology was negative.
CT abdomen (after thoracentesis):
No enlarged lymph nodes. Small amount of ascites. Large lobulated appearance to the uterus most compatible with a fibroid uterus. Hypoechoic structure in each adnexa most likely relates to the ovaries. Bowel is without evidence for obstruction. Bladder is grossly unremarkable.
What would you do about the pneumothorax after thoracentesis?
It might be worth placing a chest tube: it will drain the hydroPTx and you could check a CT scan when the lung re-expands. Furthermore, since imaging only revealed small ascites she will not have continuous large output from the CT as you would see in a hepatic hydrothorax.
BTW, was she pre-menopausal when she presented with the pneumothoraces back in 2002? Would a gyn consult be helpful to evaluate for endometriosis?
On a bit of a different note--the pleural looks a bit thick, and I would have thought that with this size of a pneumothorax she would have at least some increased sob after the procedure. If her symptoms were unchanged, than I'd be concerned about trapped lung that may not expand even with a chest tube. I think VATS with pleural biopsy might be the way to go, and a chest tube can be placed at that time...
To close out this case, I went the route of Jeff H. Partially because the PTX did not change on subsequent days after removal of fluid and she was asymptomatic. Plus, she thought I was crazy when I talked about trying a chest tube.
GYN did consult and they are getting a pelvic ultrasound. Often times, ovarian adenomas are missed on CT scan.
As an oh-by-the-way, her CA-125 was 95 (normal < 21).
Our working diagnosis is Meigs/Pseudomeigs syndrome but endormetriosis is possible.
If the ultrasound is negative, she will get a laproscopic eval of her adnexa and uterus.
As for her pleural disease, I think she is trapped. She has had blood in her pleural space for at least 3 months and she will visit with T-surg for a decortication after her GYN w/u is complete.
Any other thoughts?
Sounds like a good plan. I still like the idea of starting with a chest tube. It is still less invasive than VATS, u can send a large volume of fluid for cyto like Dan suggested and it MAY prevent the need for a VATS.
I still think that it's trapped. That's a large PTX, and it's hard to believe that someone would have no symptoms whatsoever with an acute, large PTX. The chest tube wouldn't hurt, but I doubt it would help...
Post a Commenttest post a comment