54 Y/O Male Karate instructor h/o epislepsy s/p closed head injury, depression, GERD and BPH presented w/ approximately 1-1.5 yr. h/o dyspnea w/ worsening over the past 6
months. Sx. tend to wax and wane. States that becomes SOB after walking approximately 200 ft. Also becomes quite dyspneic with stairs. Gave up martial arts 8 months ago due to dyspnea. Denies cough, occasional sputum and no hemoptysis. Denies fevers/chills/sweats, rash, joint pains/stiffness. Recent travel only to China approximately 1.5 yrs ago. Has had a recent negative HIV test. Denies unintentional wt. loss. Denies new drugs or exposures. Recent normal nuclear stress test.
ROS: occ. HA, h/o migraine, waxing and waning of GERD symptoms, denies aspiration
MEDS:
zolmitriptan
naproxen (5 pills q week)
nortryptilene
asa 81 (which he has been non-compliant w/)
omeprazole
viagra prn
Soc hx: former karate instructor, on disability for closed head injury.
No tobacco, etoh, ivda. Lives on 10 acres in Howell, MI, no farm animals, has a dog. No gardening or working in soil. No exposures w/ hobbies.
Fam hx: mom copd, heavy smoker, father- adult onset DM
PE: 124/73, 87, 93% RA
No abnormal findings on focused exam.
LABS:Normal CBC, chem 10
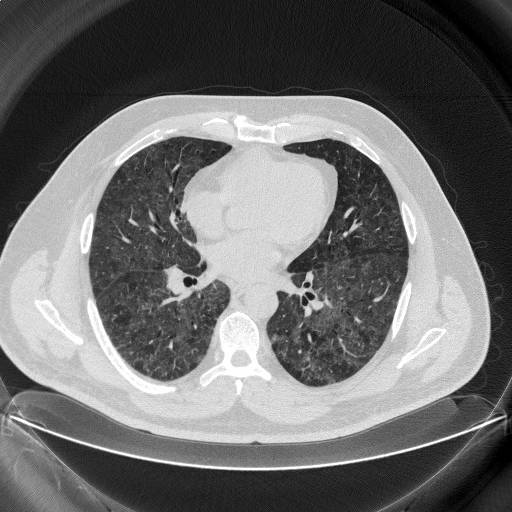
CT Thorax: Diffuse mosaic ground glass sparing only a portion of the right middle lobe. No LAD, no effusions. No real difference on inspiratory/expiratory/prone cuts. Click to enlarge:

PFT’s:
FEV1: 3.33 (80%)FVC: 3.96 (78%)TLC 89% DLCO 64%
HP and fungal panels (-)
Bronch: Cell count 150 WBC 36% lymphs 8% PMN 40% histiocytes CD4/CD8 ratio 1.7 AFB/fungal/bacterial smears/cultures (-)
TBBx: focal interstitial fibrosis, collections of alveolar macrophages and chronic inflammation. No malignancy. Negative for proteinaceous alveolar deposits.
What is your DDx and how would you proceed?
2 comments - CLICK HERE to read & add your own!:
Well, here are ome things I can think of that cause GG:
1. DIP - need open lung to confrm; he's not a smoker so maybe less likely.
2. Hypersensitivity pneumonitis - is there a correlation between any of the medications he's taking and the onset of the dyspnea? No inhalational agents are obvious from your post.
3. CHF/pulmonary edema - does he have an echo?
I would get an echo, get the medication onset history, and get an open lung. Also, some connective tissue disease can give GG/pneumonitis - like SLE; so maybe n autoimmune panel with an ANA would be helpful...
In addition to jennings comments:
Is he air trapping? Similar to DIP, RB-ILD is not likely as he is not smoking.
The BAL lymphocytosis can occur in NSIP, along with scleroderma and other collagen-vascular associated ILD's. BOOP is also a possibility.
I agree that the patient needs a surgical lung biopsy.
Post a Commenttest post a comment