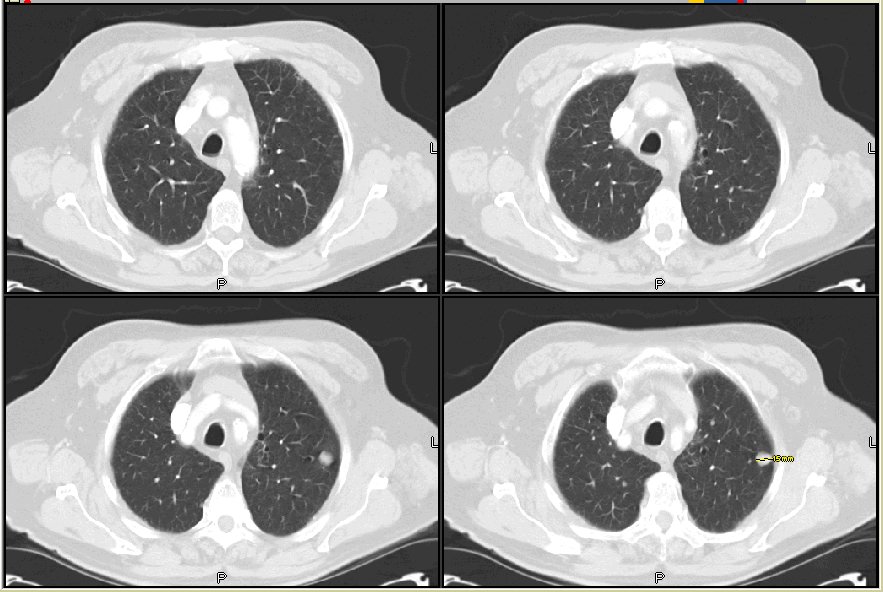
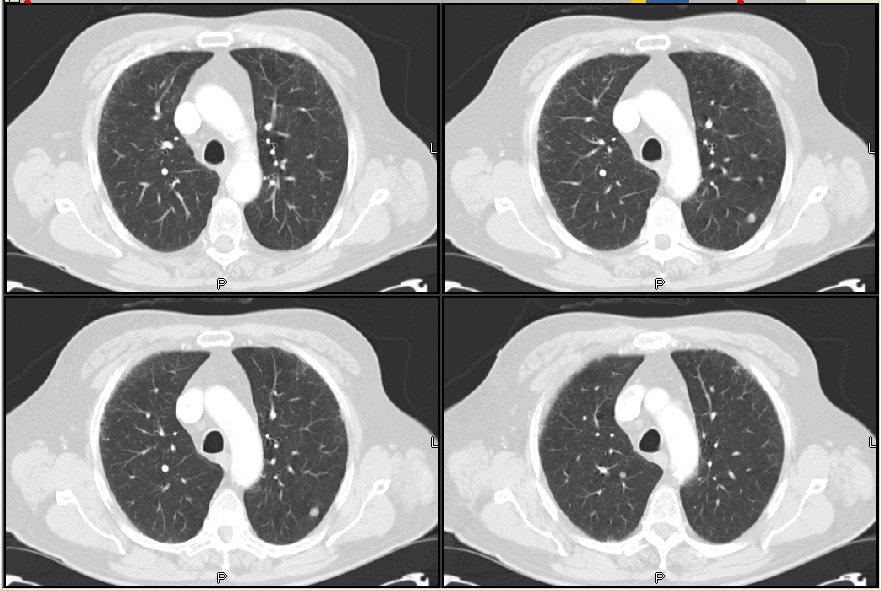
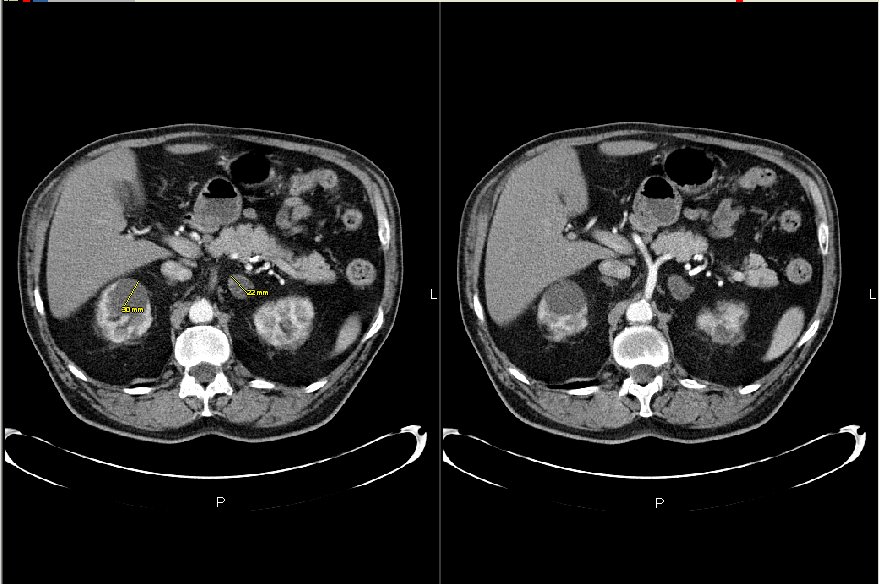
This is a 69 y/o man seen today in my office. He has very mild COPD (FEV1~75%) but continues to smoke. He had had some AECB and a CxR revealed some small pulmonary nodules. A CT scan (see below) confirmed B/L non-calcified, upper-lobe nodules (the two largest are seen on the CT slices below with no adenopathy and an adrenal mass.
I bronch'ed him and found some chronic bronchitis but nothing endobronchial. His TBBx and cyto (BAL and washings) were only significant for some inflammation. He is now assymptomatic and a PET scan showed no increased pathologic FDG-uptake anywher. What would you do next?
4 comments - CLICK HERE to read & add your own!:
was TB ruled out?
Does he have any previous CXR or CT scans to compare to?
Well, with the finding on adrenal and the nodules on chest, I agree with the ddx including TB (does fungal go to adrenal glands?) and adenocarcinoma. But with the negative PET of the adrenals, the latter is less likely actually. So I would probably do a CT-guided bx of the adrenal lesion and send it for micro (afb fungal) and pathology.
Endemic fungi can involve the adrenals. I'd biopsy the adrenals. If there is carcinoma (which I agree is less likely given the neg PET), the workup is done. If the biopsy is negative, I'd wait for the cultures and re-image, while investigating benign adrenal masses.
He did not have any infectious symptoms. He is even cough-free now. Radiology felt quite comfortable with all the various modalities of imaging that the adrenal mass was an adenoma (labs are normal).
We chose the Mendez approach: adrenal functiona was normal, sent him back to PCP for health maintenance and he is coming back in 3 months with a repeat CT scan.
Post a Commenttest post a comment