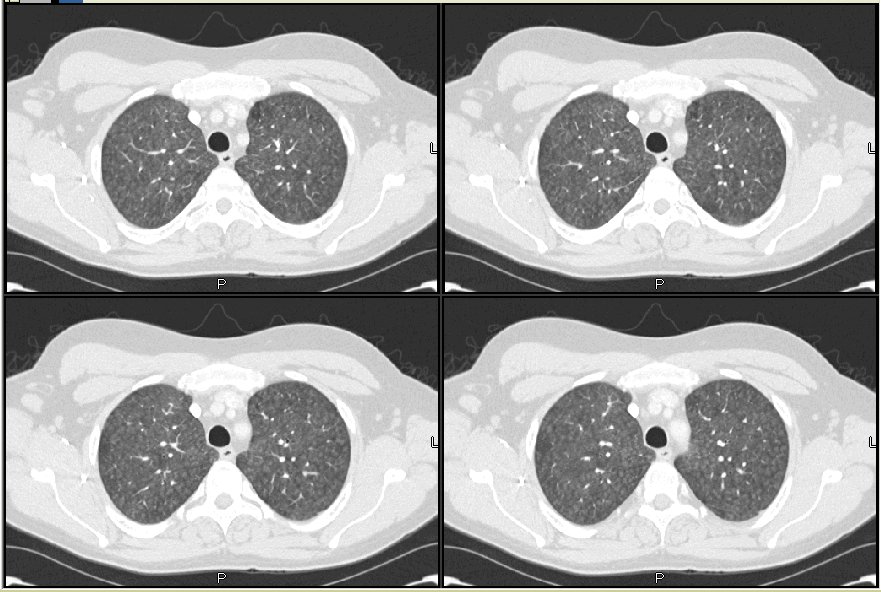
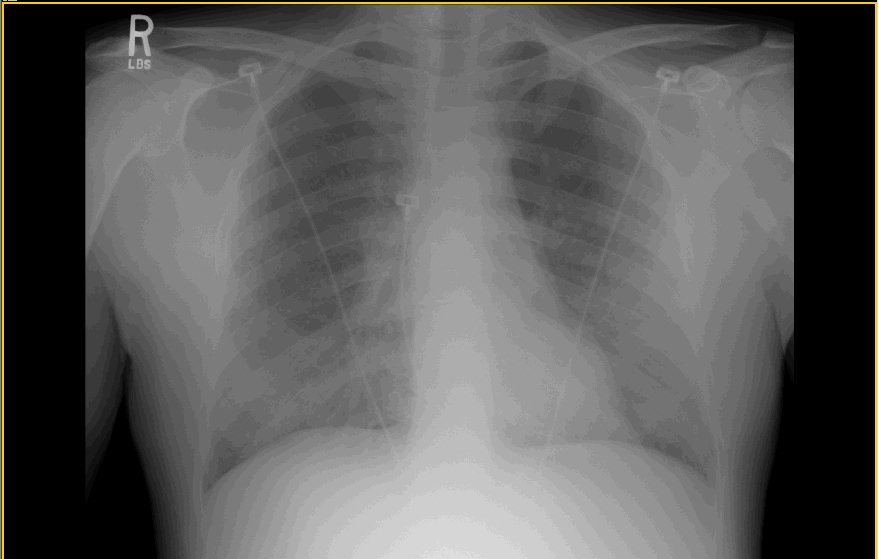
CT and CxR at that time:
Before his appointment he became more dyspneic and was admitted and we were called.
He is previously healthy. Has a dry cough, no fevers, chills, night sweats. He has some myalgias and arthralgias and dyspnea to minimal exertion.
PMHx: Unremarkable.
SHx: Smoked in the past but quit 2 years ago. He works as a mechanic and they live in a farm. He has outdoor goats and horses and two indoor cockatiels. He seems to remember that briefly before the onset of his dyspnea he opened a new bale of hay which was all moldy on the inside (not kidding).
FHx: Non-contributory.
On exam he was AAOx3 in minimal distress. POx on room air at rest was 90%, dropping with exertion. He had bibasilar crackles and inspiratory squeaks throughout. Heart, abdomen and remainder of exam was normal.
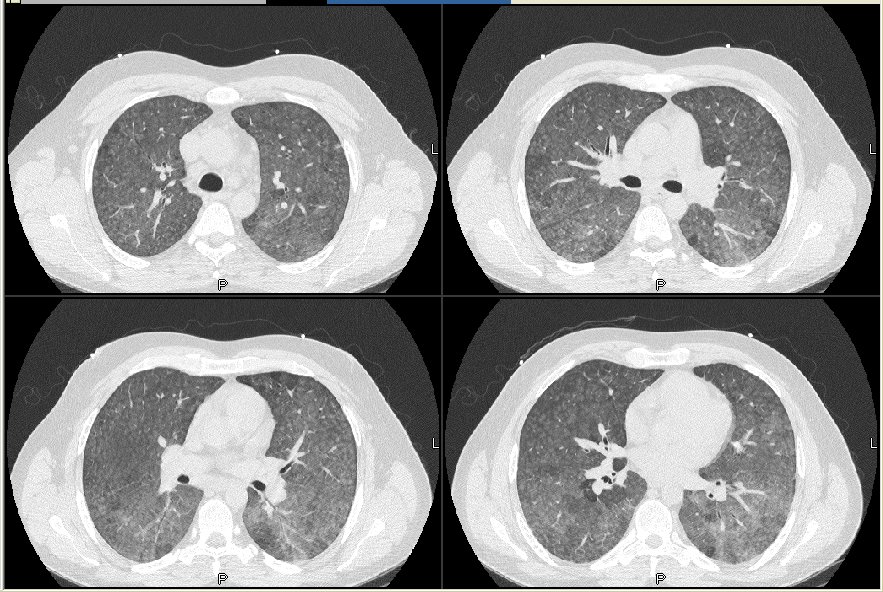
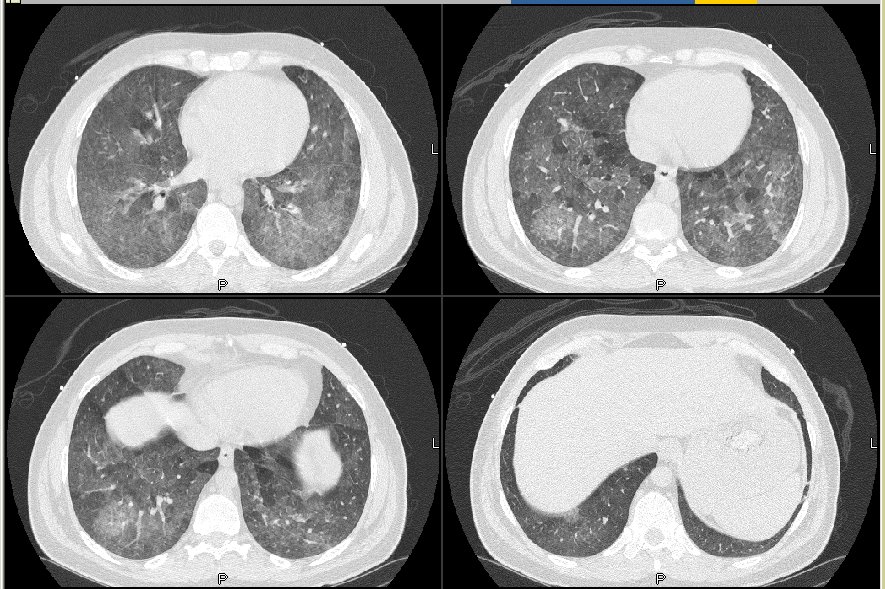
Here is his HRCT.
{kind=link}
What would you do next? What other info would you want?
3 comments - CLICK HERE to read & add your own!:
That's HP, baw. Now the only question is, is it from the cockatiels or the moldy hay. You can get a serum IgG hypersensitivity panel which would include all the common stuff (and IgG with the above history and CT scan would be enough for me). I suppose a BAL to r/o infection could be justified. An open lung to find the loose granuloma and a cell count with high cd8 ratio in my opinion would not be necessary in this patient since the diagnosis is pretty clear (assuming the serum panel is positive for thermophilic actinomycetes, or whatever the protein antigren is in cockatiel feathers...
I agree. Clinically, this is acute/subacute HP. The HRCT shows diffuse nodular ground glass. In the first CT, you've only shown us the upper lobes, which would be classic, but it is more diffuse in the HRCT.
Other possibilities in a previously healthy 39 y/o? I suppose another toxic inhalational exposure, (including cocaine/crack lung) could look like this. This seems a bit fulminant to be NSIP. DAH could look like this, although again we have no suggestive history. This is an atypical appearance for BOOP or sarcoid. PCP is a possibility; as are other (viral) opportunistic infections in the appropriate setting.
I would do a bronch, if safe, and get the CD4/CD8 (which should be less than 2, I believe, in HP),and TBBX, and I'd give a burst of steroids.
It is kind of funny how we all thought along the same lines...
He was admitted and set up for a bronch. I will post the results tomorrow in case someone else wants to add to the DDx.
Post a Commenttest post a comment