 ....
....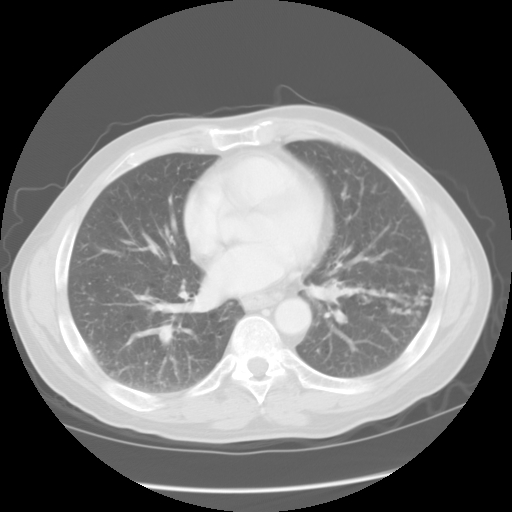 Any comments on the CT? There are 2 findings, one on each slice shown above.
Any comments on the CT? There are 2 findings, one on each slice shown above.Anyway, his cough was gone by the time of admission, and sputum could not be induced, so none could be sent. After they found him sitting in the closet, they got an LP and head MRI. LP was 22 wbc (49% L), RBC 6, gluc 51, protein 799. All micro negative (rpr,fungal,crypto,afb smear). Serum: HIV negative.
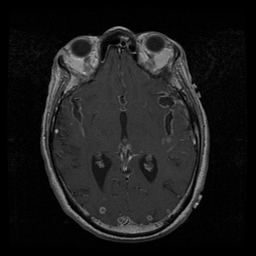
Here's the MRI.
 ...
... ...
...
What do you think and what would you recommend to the team as the next course of action?
4 comments - CLICK HERE to read & add your own!:
Jeff, could you post a higher res/bigger MR picture?
No that's what I get when I save the image to file. It doesn't give me any options for adjusting the resolution.
Well, I guess I'll have to live with the lower res image...
This is a middle-aged, unhealthy (drug abuse) man with pulmonary and CNS involvement. I didn't see anything about a TOB Hx but one bad habit often leads to another so I will assume he smokes...
The DDx based on the clinical picture alone includes TB and fungal diseases, endocarditis (sub-acute bacterial), AIDS with OI (though we now know his HIV was negative) and malignancies.
His CT scan of the chest shows these small nodules that look fuzzy when I try to blow up the picture with some focal infiltrates and what looks like some tree-in-bud changes on the preiphery in the second slice. I don't see any adenopathy and I will assume there is not much there since you excluded the mediastinal windows. These nodules could still be because of miliary TB, fungi or lymphangitic spread of a carcinoma. Septic emboli from IE and auto-immune diseases (e.g. Wegener's and other vasculitides) seem less likely on the CT scan with those smallish nodules.
His CNS pics are interesting. Those look like enhanced-T1 lesions. There are multiple ring-enhancing lesions with some meningeal enhancement. TB causes a meningoencephalitis and the LP would be consistent. However CNS tuberculoma are less common and there should be more meningeal enhancement at the base with a more posterior distribution and you did not include more basilar images. Fungal meningoencephalitis could look like this though tose are very large lesions... Metastatic carcinoma with meningeal carcinomatosis could also look like this and produce a similar LP finding. Finally lymphoma and toxoplasma could look like that though I can't tie them with the chest findings.
I would get as many cultures from different sites as possible, get and ECHO, check LFTs, check an EEG with so many CNS foci, start ABTx coverage and add some steroids (though I don't see a lot of edema on those small MR images).
To address some of your points:
1. The ring enhancing lesions are also in posterior sections.
2. There was adenopathy on the chest CT
3. Your pick-up of the nodules and your differential are correct.
4. He was ppd negative.
5. steroid were given or the brain lesions
6. a diagnostic procedure was performed.
Post a Commenttest post a comment