*. A persistent non-puritic rash in her thighs and her forearms over the same period of time.
*. Hemoptysis 2 months after the onset of DOE -– clots of blood about 1-2 teaspoons each day, then just pinkish sputum in the morning.
*. Generalized joint aches in knees, ankles, elbows, and wrist. The small joints of the hand and foot are not involved. She gives history of increased stiffness of her joints in the late afternoon. Also she has noticed increased pigmentation of her cheeks, which has been diagnosed as rosacea few months ago. She has had borderline elevated blood pressure at one of her visits at her primary care physician office.
She was referred to pulmonary clinic for this SOB. Her meds were some inhalers (she was told by her physician that her dyspnea was related to emphysema) and robitussin.
On SH, she was a smoker (PPD x 23 yrs). Occup hx non-contributory.
On exam that day, she was in no distress but SOB with speaking in full sentences.
Her weight was 126 kg. Her BMI was 42. Her SBP was 120’s.
O2 sat 81% on room air, this increased to 90% on 2l NC. RR 30. ABG on RA showed pH 7.46 CO2 33, pO2 40.8 mmHg, (hemoglobin 9.2 g). Lungs had bilateral crackles 1/3 way up. Heart sounds s1s2 no s3s4 no murmurs heard at that time. No edema. Macular patch both thighs, about 8 x 10 cm with irregular margins. Fading erythematous rash in her forearms as well. She was directly admitted from clinic because of the hypoxemia. She was in the ICU but didnt need to be intubated. CXR and some labs are shown here:

EKG sinus tach with LAE.
WBC 16 with 90% neutrophils. Hct 27. Sed rate 100. ANA negative. CK 83; c-react protein 5.7 (<5). ANCA < 20. RF negative. Chem.-7 unremark; (bicarb 23, creat 1.0). AST 60 ALT 38 albumin 4.0. HIV negative. BNP 574. Troponins elevated. D-Dimer 2000. Cardiolipin antibody: high positive IgG cardiolipin and low positive IgM cardiolipin antibody.
*****
Here is some more data, which addresses some of the points from the first comment(Arenberg):
Skin Biopsy:
Results were nonspecific, showing (in one specimen) mild telangiectasia and rare vessels without inflammation and in other slices this: "interstitial histiocytic infiltrate noted throughout the dermis. This is associated with focal increased dermal mucin as confirmed with Alcian blue stain. There is also an infiltrate
of eosinophils. In rare areas there is basophilic degeneration of collagen bundles with surrounding neutrophilic debris containing erythrocyte thrombi. Direct immunofluorescence study was negative.
Other lab tests:
Hepatitis C was negative. Complements C3 and C4 were normal. The U/A was normal without casts or protein. In terms of your thoughts on it being a vasculitis with pulmonary hemorrage, a bronch was done. Serial BAL was indeed bloody, but although the bronchoscopist felt that the bloody color did NOT change after 3 serial lavages, a hematocrit on these lavages was not done to confirm this impression. Nonetheless, the micro from the BAL was negative. The cell count was about 2850 WBC's, with 78% lymphs on lavage 1 and 80% neutrophils on lavage 2!
Here is a CT before and after treatment with BOTH lasix and steroids.
 before
before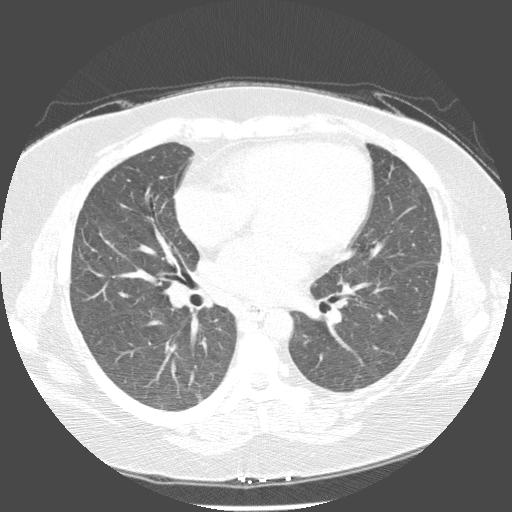 after
afterWhat is your ddx now, and what other tests would you like to help confirm?
*****
Note: this case has a follow-up. Please read that post after checking out the comments here.
4 comments - CLICK HERE to read & add your own!:
Great case and great DDx by Arenberg. Vasculitis was also very high on my DDx with skin involvement and pulmonary hemorrhage (+ high ESR and anemia that seems to combine blood loss and chronic dz).
Antiphospholipid Ab synd may present with pulm hemorrhage and skin rashes by itself.
Other collagen vascular diseases may also be associated with a capillaritis and may be ANA neg. I would add to the laundry list an Anti-Scl70, Anti-uRNP1 (MCTD) and even throw in an anti-centromere and Anti-SSA/SSB. You listed a very bland U/A so you might be trying to dissuade us from and anti-GBM Ab...
Any recreational drug use?
As an infectious DDx (doubtful) I will mention sub-acute infectious endocarditis which may have quite dramatic immune phenomena with negative serologies.
Very interesting case, and that's a remarkable change in the CT scan. What was the dose/duration of steroid given?
I agree that this is probably some type of vasculitis with alveolar hemorrhage. My question is where to go from here? Is this someone who needs cytoxan, or do we treat with steroids alone. So, I'd get the additional studies mentioned by Carlos.
I went to another post for followup.
http://pulmonaryroundtable.blogspot.com/2005/09/follow-up-to-hypoxemia-and-diagnostic.html
Post a Commenttest post a comment