 . (An abdominal CT in 2003 showed the lung cuts were negative.)
. (An abdominal CT in 2003 showed the lung cuts were negative.) In November of 2004 a follow-up CT
 showed that there was still a residual opacity in the lung abutting the pleura. He was no longer symptomatic. A bronch was done; airway exam was unremarkable. Micro and cyto were negative. A repeat CT 3 months later
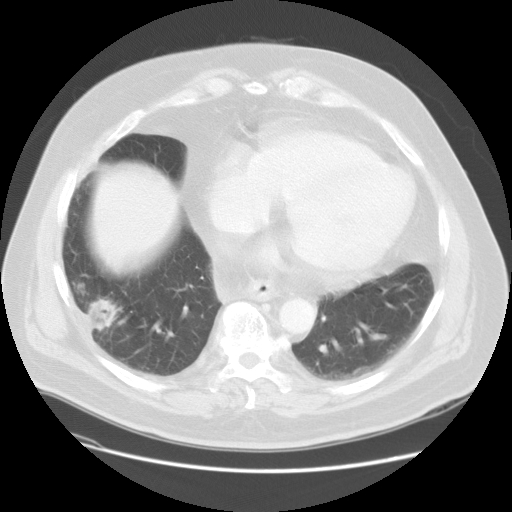
showed that there was still a residual opacity in the lung abutting the pleura. He was no longer symptomatic. A bronch was done; airway exam was unremarkable. Micro and cyto were negative. A repeat CT 3 months later 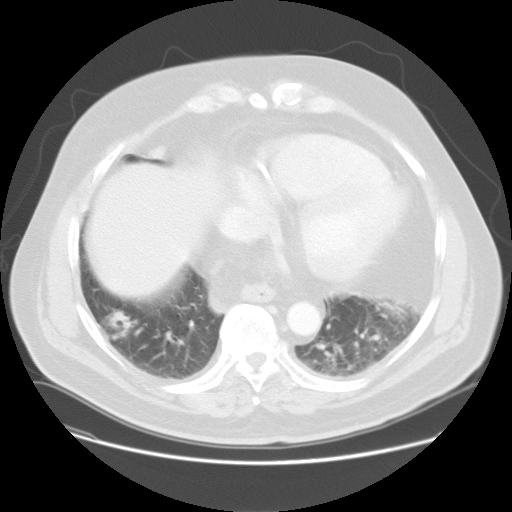 showed persistent opacity in the RLL; there was the nodular opacity in the right lower lobe measuring 2.1 cm x 2.1 cm. There was no significant change in the size, but surrounding areas suggested some resolution making an inflammatory process possible. This month he developed a bit of hemoptysis and was hospitalized briefly. A repeat CT done this month
showed persistent opacity in the RLL; there was the nodular opacity in the right lower lobe measuring 2.1 cm x 2.1 cm. There was no significant change in the size, but surrounding areas suggested some resolution making an inflammatory process possible. This month he developed a bit of hemoptysis and was hospitalized briefly. A repeat CT done this month  showed size now 3.4 cm x 2.1 cm with a central area of cavitation. Because he is a Jehovah's Witness and didn't want surgery (surgery said they would take it out if the patient wanted it), a core needle CT guided bx was done. It showed "1. Reactive fibrosis with chronic inflammation 2. Negative for a neoplastic change." Micro was not sent (!) but no organisms seen under histo at least.
showed size now 3.4 cm x 2.1 cm with a central area of cavitation. Because he is a Jehovah's Witness and didn't want surgery (surgery said they would take it out if the patient wanted it), a core needle CT guided bx was done. It showed "1. Reactive fibrosis with chronic inflammation 2. Negative for a neoplastic change." Micro was not sent (!) but no organisms seen under histo at least.What would you do now?
4 comments - CLICK HERE to read & add your own!:
Well, the lesion seemed to be getting more lucent between scans which I guess is consistent with the early impression of some resolution. Lung cancer is fairly low on my DDx (non-smoker, lower-lobe, initial decrease in size) but a met from elsewhere is still possible. I think JJ might be steering us towards an inflammatory process and that would be my impression too. You could try some ABTx that would cover indolent mixed-flora and anaerobes (such as blood-free Augmentin) for a few weeks and repeat a CT within 4 weeks. It might be too soon for a change in a malignant lesion but not for an inflammatory lesion and any resolution would help. Or you could consider repeat sampling (bronch) with more Cxs and hope for an actual Dx.
So I guess no one's worried about this being cancer? I'm not too concerned either except for the growth; perhaps it's something like actinomycetes, given the pleural based lesion, but no one here would opt to take it out?
Doug's suggestion of WG is a good one, especially in lieu of his episode of hemoptysis. Have you ever examined his urine for dysmorphic RBC's?
I think a repeat bronch is very low yield in this patient and would not do it.
Similar to other suggestions, I would be very nervous leaving this thing in his chest given its increase in size. If he is not willing to have it resected, why get serial CT scans?
I agree that the likelihood of carcinoma in this patient is relatively low, and there is not much clinically to support an infectious disease (although mycobacterium, actinomycetes, nocardia, staph) would be possibilities.
Another thought would be that the patient had a lung abscess; these may take months of antibiotics to resolve, and even while on antibiotics will frequently look worse radiographically before getting better.
My first option would be resection; if the patient remains resistant to that, I would treat for three months with Clindamycin or Augmenting, then repeat imaging.
Post a Commenttest post a comment