This 53 year old executive for a large multinational was referred for a second opinion regarding some asthma and hypoxemia. He had been very healthy until abouit 9 months ago when a routine physical exam resulted in a hemoglobin level of 18 g/dl, and was also abnormal when repeated. He was sent to see a hematologist, but did not follow up until more recently as he had been feeling well. He travelled to Brazil (his country of origin, this is for Carlos, he wanted to get some decent Feijoada...that and his Mom died of COPD...feel free to edit this part out). While there he developed a dry cough that persisted upon return, and eventually was treated with several courses of outpatient antibiotics, and steroids.
He was referred to see a pulmonologist, who noted his O2% sat was low (~90-92), and referred him to the hospital, wehere a blood gas revealed a PO2 of 60 and a sat of ~85%. He had an extensive workup including a PE protocol CT which revealed no clot, a high resolution CT of the chest with normal lungs (no ILD, no nodules, no emphysemetous lung). The only abnormality was on the images included (see jpeg). He was also noted to have a hemoglobin of 18.5, but normal WBC count & differential. Electrolytes, usine, and muscle enzymes were normal (although his CK was in the upper reach of the normal range) He was treated with steroids and eventually discharged without a diagnosis, but was told to see us, and that he would need some follow up for the incidental abnorrmality on his CT.
He had an echocardiogram which revealed normal LV function, no shunt, and minimal tricuspid regurgitation with "mild pulmonary hypertension" but no estimetd RVSP was reported.
On review of systems he specifically mentioned a fatigue, and some weakness in his legs, as well as a frequent sensation of "choking" on saliva or food, nut no frank aspiration. He had just had a sleep study the week before he came down to Ann Arbor, and was told it was positive. He does have symtoms of poor quality sleep, but no PND, orthopnes, fevers, chills, or abdominal complaints. He has lost about 10 pounds in the last 6 months.
Since discharge from the hospital he has felt slightly improved, but he was briefly re-hospitalized for three days with atrial fibrillation, which spontaneously converted after rate control.
He had a normal physical exam except for some steroid induced acne (my guess, remember I am married to a dermatologist), and was a fit 5' 6" tall and 160# (not obese)
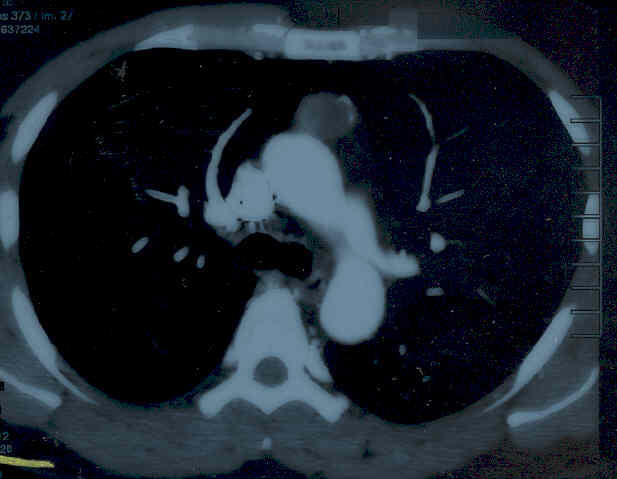
His spirometry was completely normal when I saw him, and his O2 sat was 97% on room air. The image included is a representative cut showing the abnormality.
What is the differential for this finding, and how (if at all) would you connect this with his fatigue hypoxemia, and his elevated hemoglobin?
What test(s) would you order next? I have no clue, but I know what I did. This is a work in progress, so as I get his results back I'll send them along.
Update above.
8 comments - CLICK HERE to read & add your own!:
Thanks for the case DA. So, a 53 y/o previously healthy man with hypoxia, fatigue, subjective weakness, some degree of pulmonary hypertension, and normal pulmonary mechanics.
The CT scan shows something anterior to the arch of the aorta. I don't know what that is, but it looks like it has some heterogenous attenuation and a "whiff" of either contrast or calcium. It looks contuguous with the aorta, but doesn't seem to be invading. Also, this is only one cut but there does seem to be an anomolous (?spelling?) vessel coming off of the aorta-same attenuation, and it doesn't look right for the PA.
He has no s/s to suggest an infection. As you stated, there is no parenchymal abnormality noted on the prior CT scan, and nothing suspicous for PE.
So, two possibilities come to mind here. 1) If that is contrast material, there would be a left-right shunt: this could cause pulmonary hypertension, but shouldn't cause the hypoxia unless the right sided pressures were so elevated that there was Eisenmenger's physiology. The prior echo did not seem consistent with that.
2) If that is calcium, I'd wonder about old granulomatous disease and consider fibrosing mediasteinitis.
Of course, I may be over-calling all of this... I think I'd repeat an echo here to get a better sence of the pulmonary hypertension, and then consider a PA-gram and an aortogram to further define the vascular anatomy. I suppose an MRA of the great vessels could be done first. If all of that is negative, I'd consider a mediasteinoscopy.
I'm very interested to see what others think, as all of this is a shot in the dark!
I agree with JH about the close abuttment of the abnormalitiy to the ascending aorta. It is concerning for a sacular aneurysm. The angle of the lower edge suggests it may be coming from the aorta and the lack of contrast may indicate clot. I would confirm this impression with a radiologist and if agreed, would go to a TEE to confirm this.
I think that the results of the sleep study are crucial here. Positive may mean anything and you will need the report. It will be very significant if the result shows severe sleep apnea, with severe desaturation (which would explain the polycythemia from chronic hypoxia). is this a morbidly obese man? BMI? is obesity hypoventilation a possibility here? was there hypercapnea on his ABG? what was the A-a gradient?
The opacity anterior to the aorta is a different problem and will need separate workup.
A couple of thoughts.
First, if he has severe OSA, he could get hypoxic vasoconstriction, pulmonary hypertension and hypoxemia with exercise. So, that sleep study would be helpful. I know better than to ask a Wed clinic man if you measured his neck circumference and graded his airway with Mallampati classification.
Second, I think full PFT's would be very helpful. A low DLCO in the absence of any PE would pretty much r/i pulmonary hypertension. Then, we would need a diagnosis.
To figure that out, I would MRI/MRA his chest to get a better idea on what that anterior abnormality is. I think I would avoid mediastinoscopy until you figure out if is vascular or not. Maybe Jennings could reconstruct the CT to see the vascular supply.
If the MRI/MRA is negative, I would do a right heart cath. While there, I would do both pressure measurements and saturations in the SVC, RA, RV and pulm artery.
I'll also take the blame for leading the discussion astray with my vascular abnormality hypothesis. I'll also take the hint, and speculate that this may be a "simple" anterior mediastinal mass...
Of course, I will point out that my initial post said that, if this were calcium and not a vascular lesion, than I would push for a mediastinoscopy. I still hold to that, and now think that tissue is the issue.
Ok then with anterior mediastinal mass and fatigue I will ask what his Mips and MEPs are in case this is thymoma-related myasthenia. Other options include germ cell, with teratoma being one that can give you calcification.
I missed the part mentioning about his body habitus.......so obviously OHS is not an issue here. I would still attempt to obtain the report of the sleep study, to know what is his apnea/hypopnea index and also learn about the extent of the nocturnal desaturation (which happen both with apneas and hypopneas)..you have nothing to lose, and I am sure that you have been surprised many times to find severe sleep-disordered breathing in people without the typical body habitus. PFT is a great idea, and I would include with that muscle forces especially if he had hypercapnea on his ABG.
in regards to the anterior mediastiastinal opacity, one way to tie all this together would be to think of thymoma causing myasthenia gravis(as the author reported weakness/choking on food..) which can be associated sometimes with red cell aplasia (hence the polycythemia).....
I would get erythropoietin level, get neuro eval for myasthenia/serologic evaluation.
Hypoxemia will cause a secondaryerythrocytosis too and this need not be polycythemia. I don't remmember anterior mediastinal masses causing polycythemia... renal cell Ca can lead to increased erythropoetin and polycythemia and may certainly metastasize to the chest though that does not look like a typical renal cell met.
With his body habitus and AHI I would not expect persistent PHTN during the day. I may have missed but was he hypercapnic?
Post a Commenttest post a comment