85F with history of mucoepidermoid cancer of the
salivary gland treated with chemo and RT about 4 years
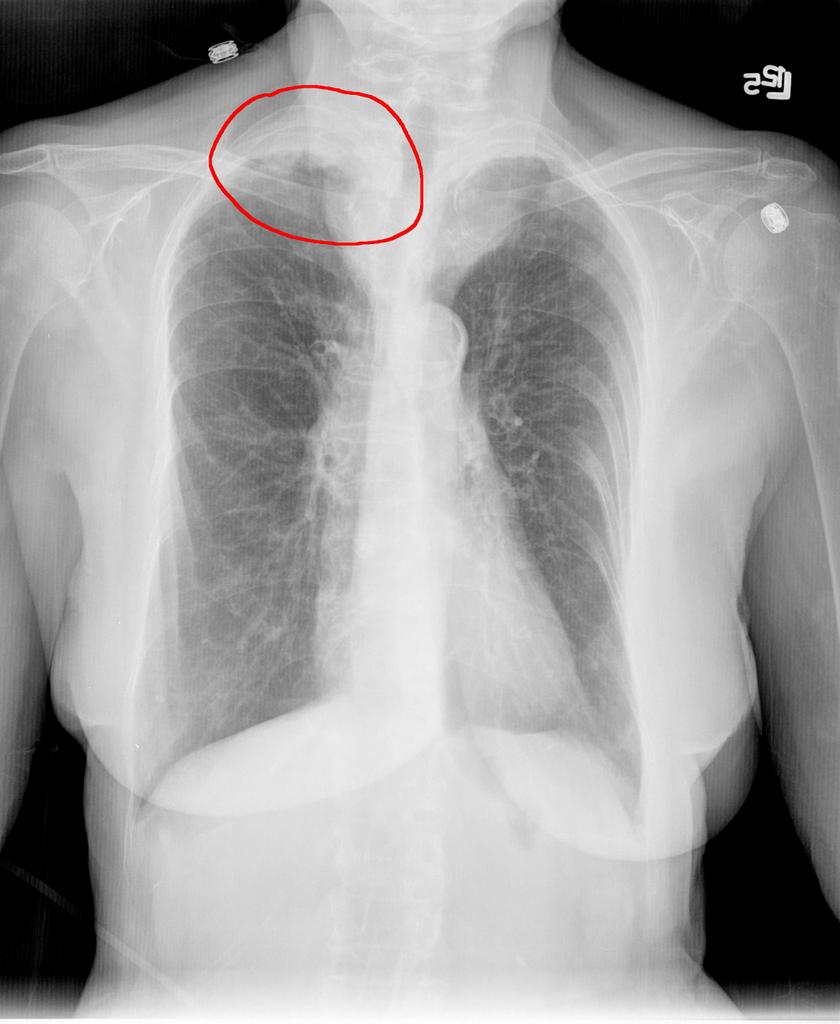
ago. Routine follow up chest xray shows new RUL mass
like abnormality in the apex abutting the pleura. CT
guided biopsy was nondiagnostic. Sputum sample that
was done intially to rule out TB grew Rhodococcus
Gordona.
How would you treat this? The finding was incidental
and thought to potentially be malignancy.
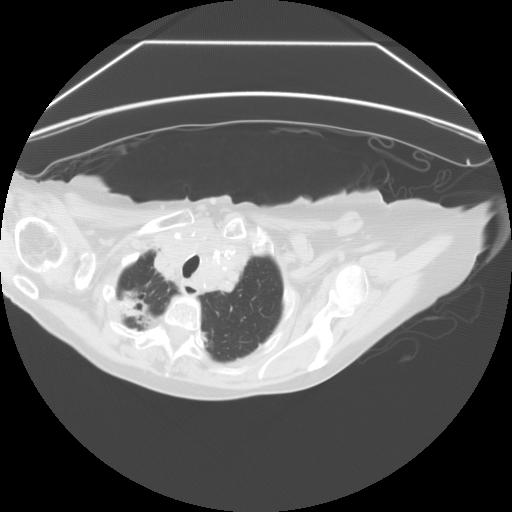
Here is a CT. It was not thought to be cavitary based on radiologists interpretation.
5 comments - CLICK HERE to read & add your own!:
Rhodococcus is an interesting agent. Though it's a GPC it is an intracellular pathogen that behaves like Nocardia: it usually causes granulomatous infection in the upper lobes of immunocompromised patients. It is not a common isolate so it is usually regarded as a pathogen particularly if tissue shows granulomata formation.
The major species is R. equi, which as the name suggests is a pathogen and colonizer of horses and other herbivores and disease is usually associated with exposure to horses or farms.
Rhodococcus has several species and subtypes but I don't remember R. gordona as one of them... besides Mycobacteium gordonae, there is a genus of intracellular organisms called Gordoniae that likes to bahave like Nocardia and Rhodococcus.
Treatment of rhodococcus as I remember is a pain in the neck. It is a rare GPC that does not respond to vanco (it is SS in vitro though) and it requires a couple of drugs for a while. I would ask the pathologists to comment on the tissue from the Bx whether there was any granulomata.
As I read this, there is no tissue to examine; this was from a sputum sample.
I've just been trying to look up information on Rhodococcus Gordona, and as best as I can find, these are two closely related, but distinct, species. I agree that rhodococcus is typically considered a pathogen, and it can be isolated in sputum. However, according to UptoDate, little is known about the pathogenic potential of non-equi rhodococcus. Further, R.equi is an opportunistic pathogen, and it doesn't sound as if this patient is immunocompromised. Most cases in non-immunocompromised adults are associated with cavitary lesions. So'd I'd be interested to know if this is R. equi or another species.
I think that prior to treatment, I'd get a CT scan (?pneumonia, cavitation, lympadenopathy, or other evidence of active infection) and follow it with a bronch with BAL/biopsy to get cultures and to look for granulomata.
R. equi is usually resistant to penicillins and cephalosporins. R. equi is usually susceptible in vitro to erythromycin and extended spectrum macrolides, rifampin, fluoroquinolones, aminoglycosides, glycopeptides, and imipenem. If treatment is started, an extended-spectrum macrolide is recommended for immunocompetent patients. For immunocompromised patients, combination therapy is recommended. I did not find firm recommendations for duration of therapy: at least two months for immunocompromised patients was recommended by UpToDate.
The immunocompromise for Rhodococcus disease can be broader than say for PCP. It is more like Nocardia or Actino in the sense that people who are chronically ill (such as a seemingly thin 85 y/o man with previous malignancy and Chemo/XrT) and/or have underlying lung disease. My suggestion on the path was Re: the CT-guided Bx. Though the Rhodococcus was found in sputum the samples from the Bx might add some info (such as presence of chronic inflammation).
I agree with Jeff that a CT would be very informative.
Interesting. I am inclined to believe the Rhodococcus is real... It might be worth doing a bronch with some TBBx and BAL of the area.
Post a Commenttest post a comment