This 36 year old woman with no past medical history presented with 4-5 months of gradually increasing dyspnea on exertion. Her episodes of DOE progressed to occur with minimal exertion such as dressing. Her review of systems include:
*. A persistent non-puritic rash in her thighs and her forearms over the same period of time.
*. Hemoptysis 2 months after the onset of DOE -– clots of blood about 1-2 teaspoons each day, then just pinkish sputum in the morning.
*. Generalized joint aches in knees, ankles, elbows, and wrist. The small joints of the hand and foot are not involved. She gives history of increased stiffness of her joints in the late afternoon. Also she has noticed increased pigmentation of her cheeks, which has been diagnosed as rosacea few months ago. She has had borderline elevated blood pressure at one of her visits at her primary care physician office.
She was referred to pulmonary clinic for this SOB. Her meds were some inhalers (she was told by her physician that her dyspnea was related to emphysema) and robitussin.
On SH, she was a smoker (PPD x 23 yrs). Occup hx non-contributory.
On exam that day, she was in no distress but SOB with speaking in full sentences.
Her weight was 126 kg. Her BMI was 42. Her SBP was 120’s.
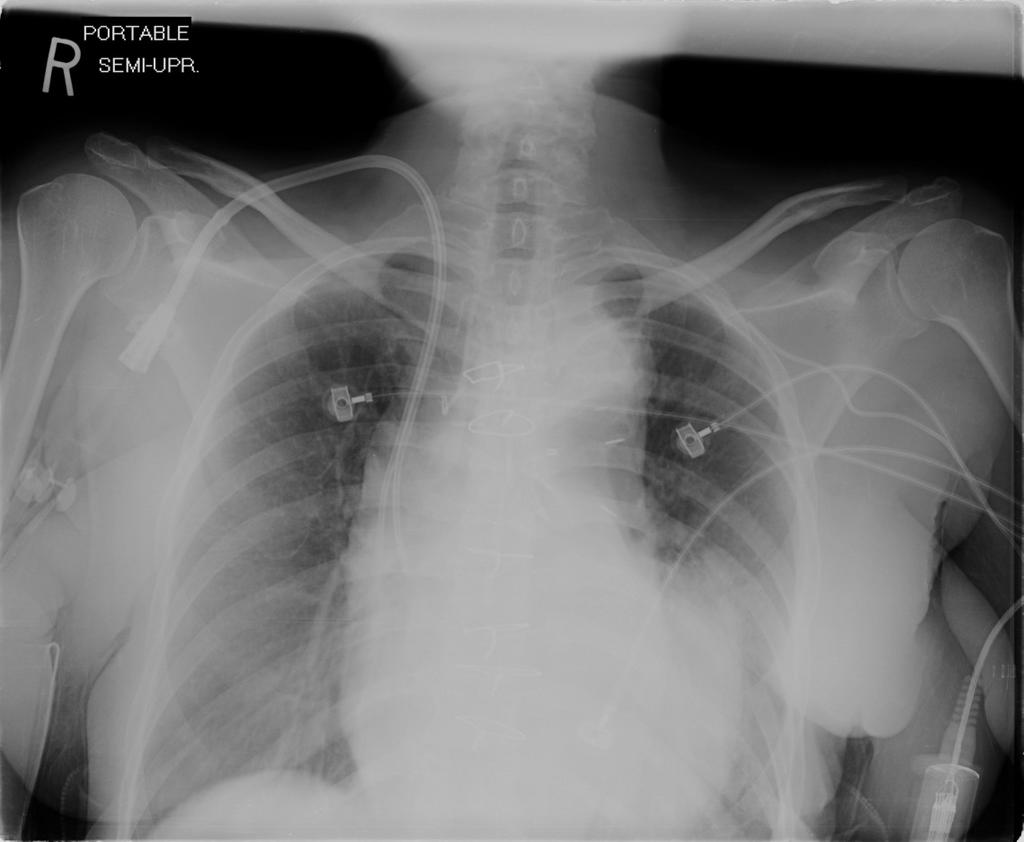
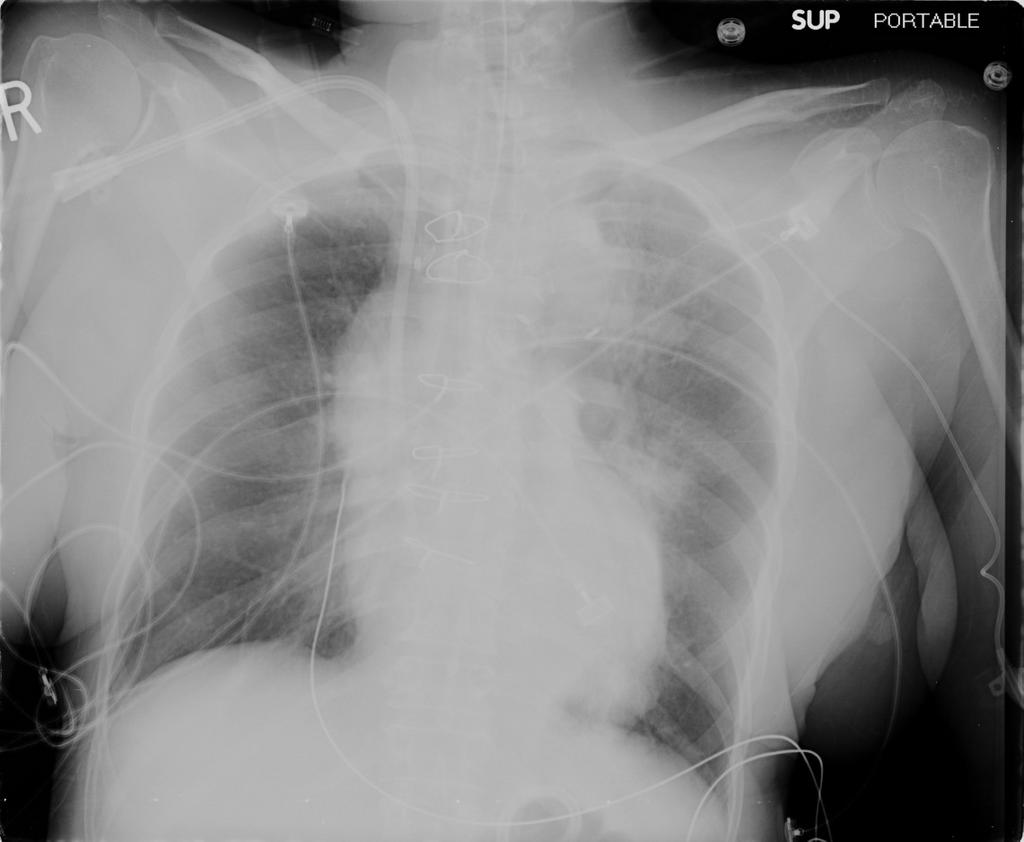
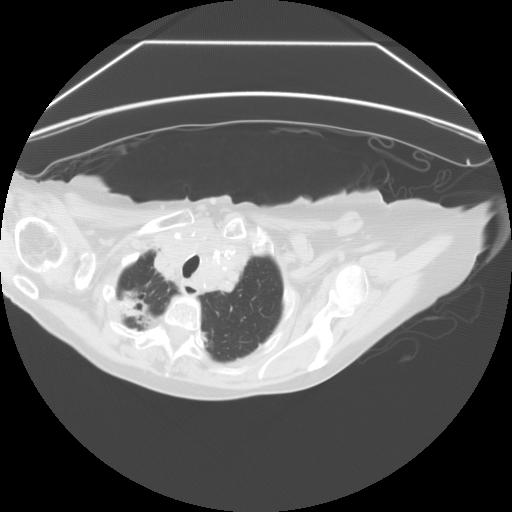
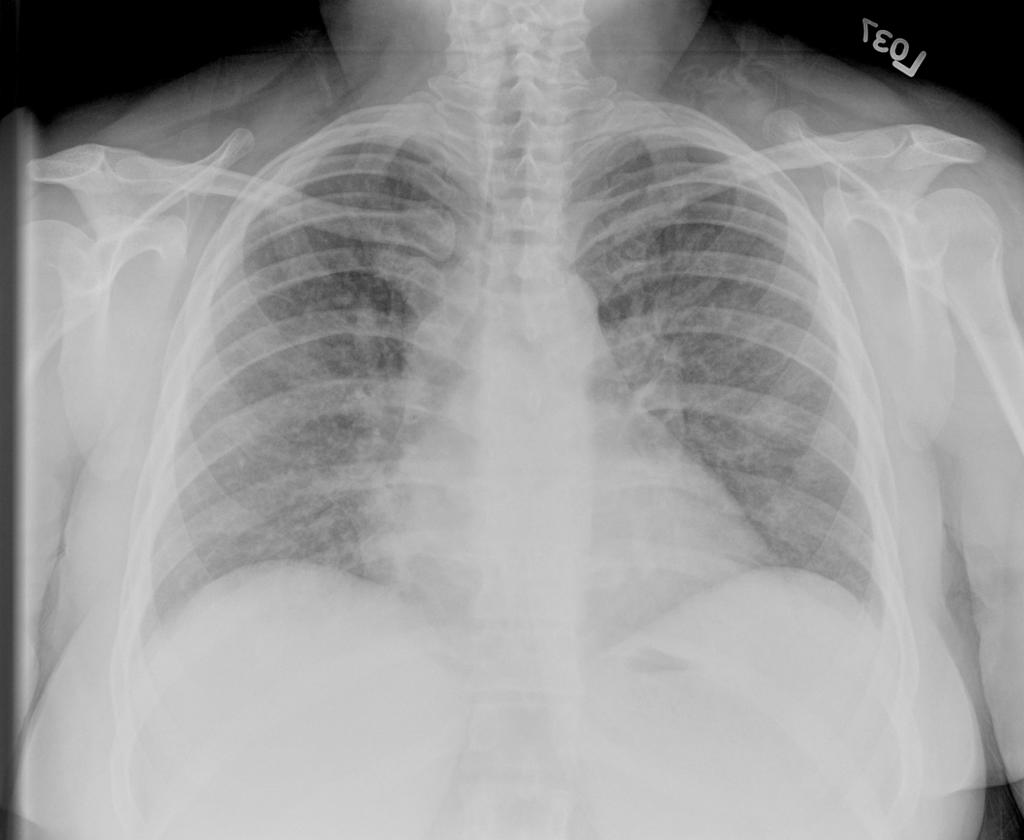
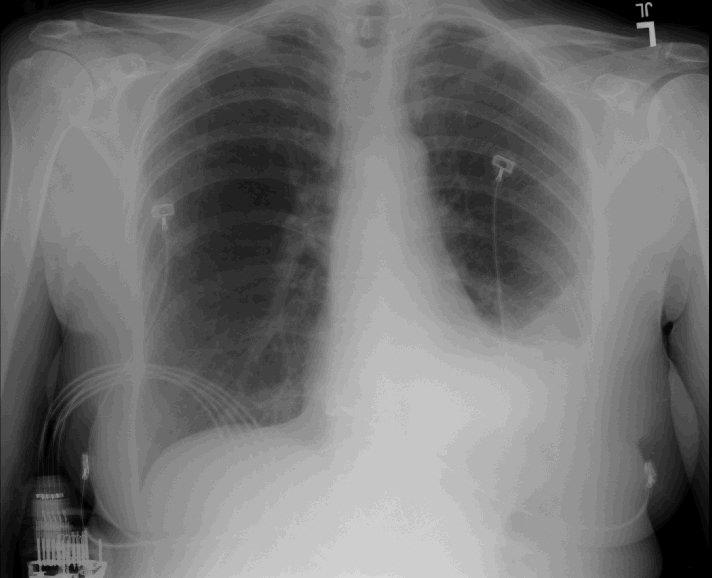
O2 sat 81% on room air, this increased to 90% on 2l NC. RR 30. ABG on RA showed pH 7.46 CO2 33, pO2 40.8 mmHg, (hemoglobin 9.2 g). Lungs had bilateral crackles 1/3 way up. Heart sounds s1s2 no s3s4 no murmurs heard at that time. No edema. Macular patch both thighs, about 8 x 10 cm with irregular margins. Fading erythematous rash in her forearms as well. She was directly admitted from clinic because of the hypoxemia. She was in the ICU but didnt need to be intubated. CXR and some labs are shown here:

EKG sinus tach with LAE.
WBC 16 with 90% neutrophils. Hct 27. Sed rate 100. ANA negative. CK 83; c-react protein 5.7 (<5). ANCA < 20. RF negative. Chem.-7 unremark; (bicarb 23, creat 1.0). AST 60 ALT 38 albumin 4.0. HIV negative. BNP 574. Troponins elevated. D-Dimer 2000. Cardiolipin antibody: high positive IgG cardiolipin and low positive IgM cardiolipin antibody.
*****
Here is some more data, which addresses some of the points from the first comment(Arenberg):
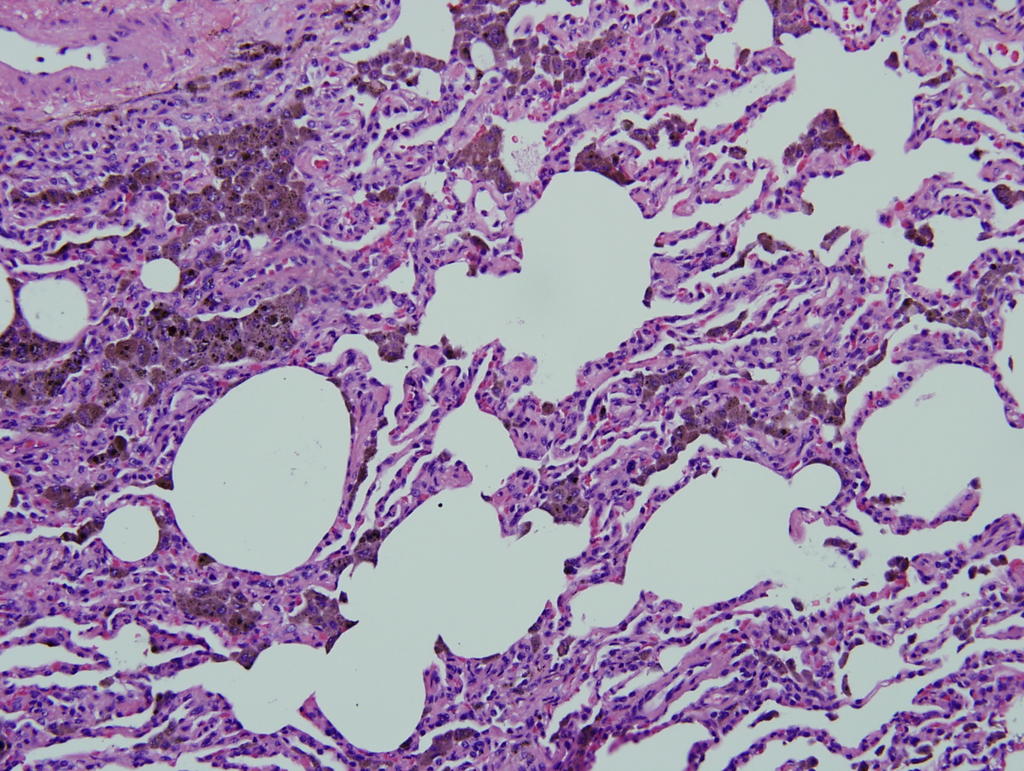
Skin Biopsy:Results were nonspecific, showing (in one specimen) mild telangiectasia and rare vessels without inflammation and in other slices this: "interstitial histiocytic infiltrate noted throughout the dermis. This is associated with focal increased dermal mucin as confirmed with Alcian blue stain. There is also an infiltrate
of eosinophils. In rare areas there is basophilic degeneration of collagen bundles with surrounding neutrophilic debris containing erythrocyte thrombi. Direct immunofluorescence study was negative.
Other lab tests:Hepatitis C was negative. Complements C3 and C4 were normal. The U/A was normal without casts or protein. In terms of your thoughts on it being a vasculitis with pulmonary hemorrage, a bronch was done. Serial BAL was indeed bloody, but although the bronchoscopist felt that the bloody color did NOT change after 3 serial lavages, a hematocrit on these lavages was not done to confirm this impression. Nonetheless, the micro from the BAL was negative. The cell count was about 2850 WBC's, with 78% lymphs on lavage 1 and 80% neutrophils on lavage 2!
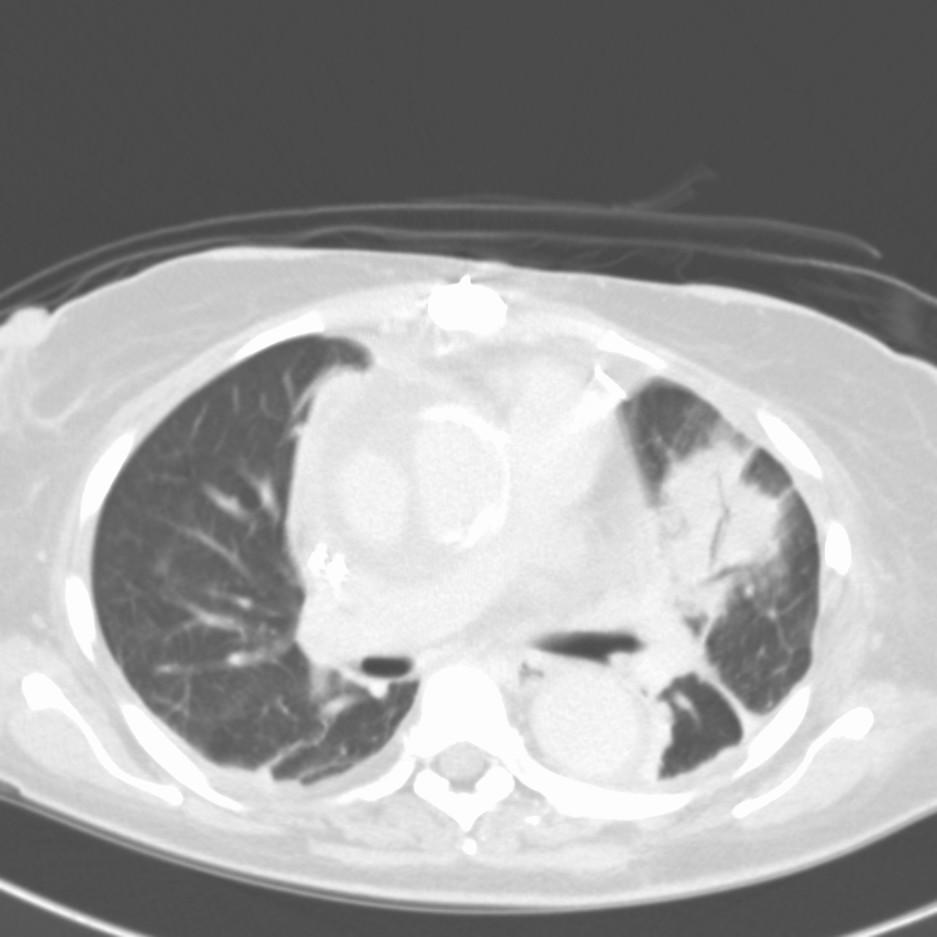
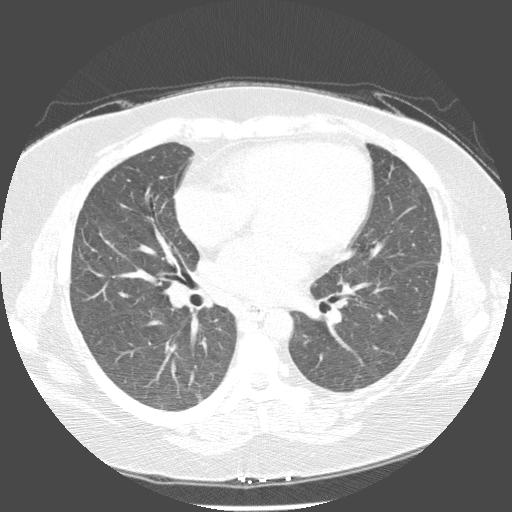
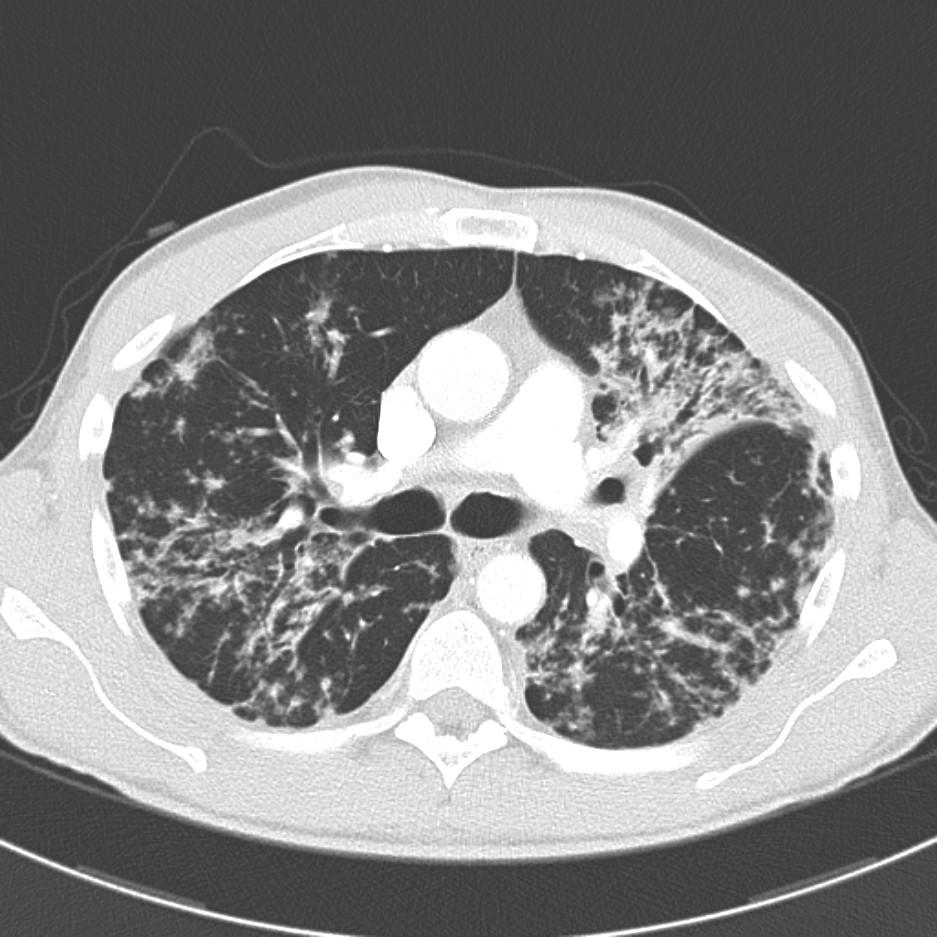
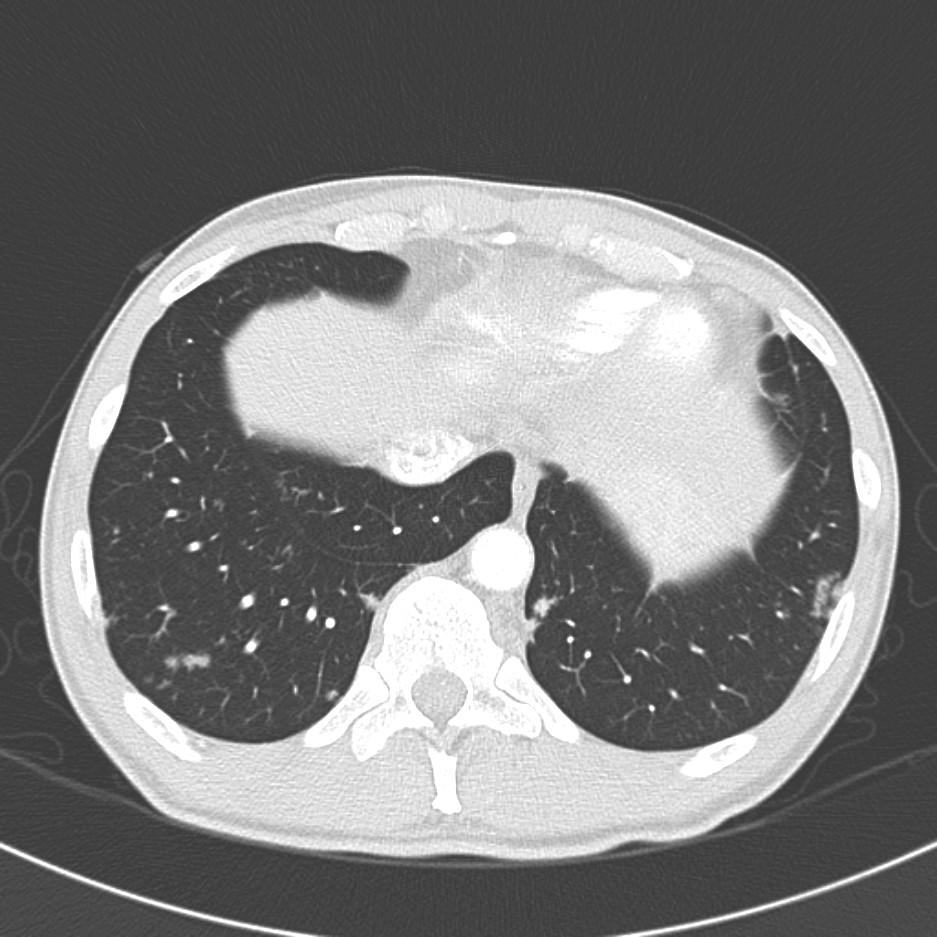
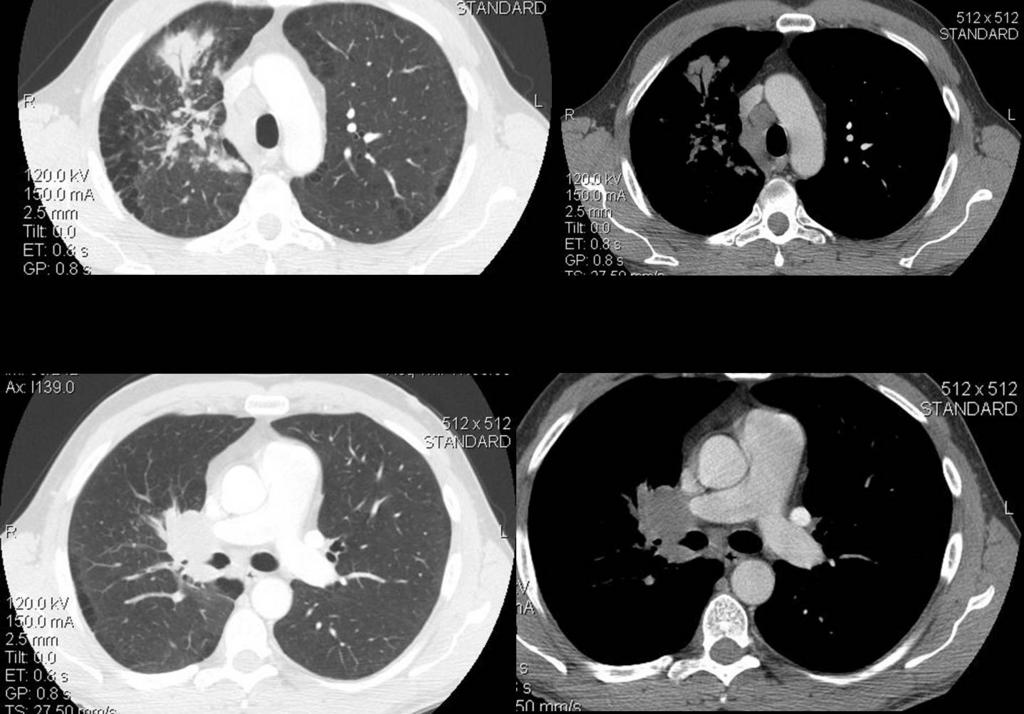
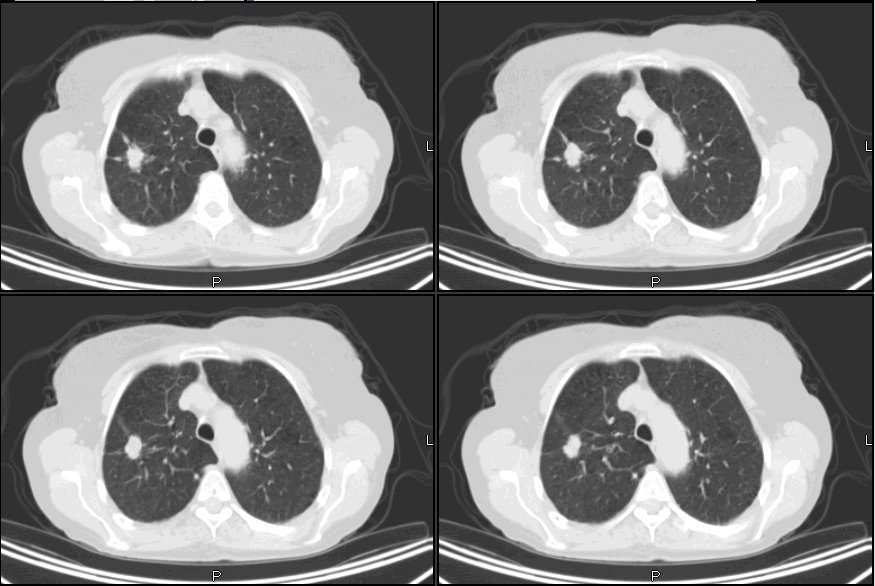
Here is a CT before and after treatment with BOTH lasix and steroids.
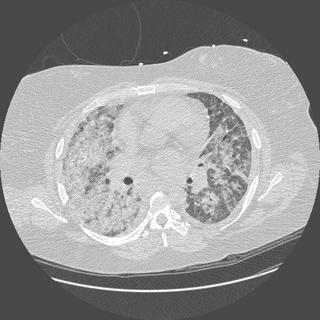 before
before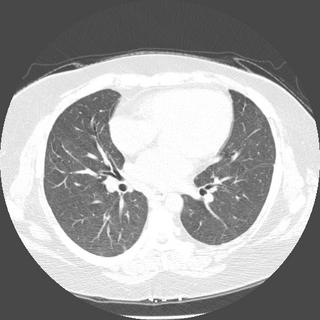 after
afterWhat is your ddx now, and what other tests would you like to help confirm?
*****
Note: this case has a follow-up. Please read that post after checking out the comments here.
 . (An abdominal CT in 2003 showed the lung cuts were negative.)
. (An abdominal CT in 2003 showed the lung cuts were negative.) 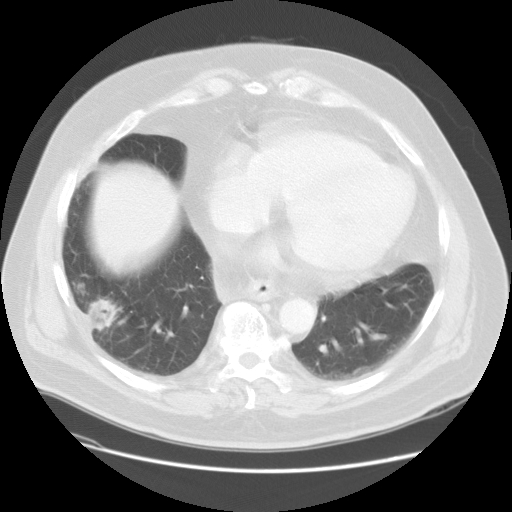 showed that there was still a residual opacity in the lung abutting the pleura. He was no longer symptomatic. A bronch was done; airway exam was unremarkable. Micro and cyto were negative. A repeat CT 3 months later
showed that there was still a residual opacity in the lung abutting the pleura. He was no longer symptomatic. A bronch was done; airway exam was unremarkable. Micro and cyto were negative. A repeat CT 3 months later 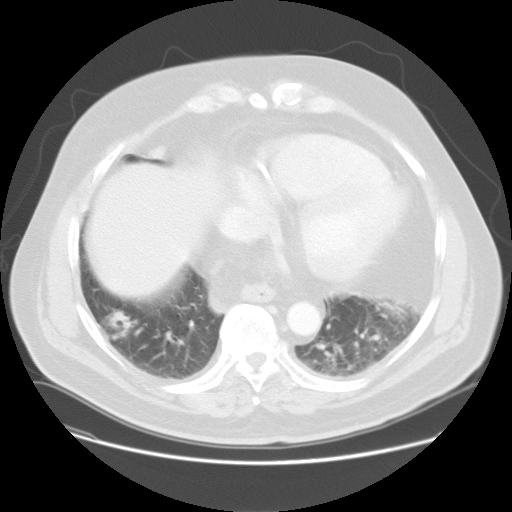 showed persistent opacity in the RLL; there was the nodular opacity in the right lower lobe measuring 2.1 cm x 2.1 cm. There was no significant change in the size, but surrounding areas suggested some resolution making an inflammatory process possible. This month he developed a bit of hemoptysis and was hospitalized briefly. A repeat CT done this month
showed persistent opacity in the RLL; there was the nodular opacity in the right lower lobe measuring 2.1 cm x 2.1 cm. There was no significant change in the size, but surrounding areas suggested some resolution making an inflammatory process possible. This month he developed a bit of hemoptysis and was hospitalized briefly. A repeat CT done this month  showed size now 3.4 cm x 2.1 cm with a central area of cavitation. Because he is a Jehovah's Witness and didn't want surgery (surgery said they would take it out if the patient wanted it), a core needle CT guided bx was done. It showed "1. Reactive fibrosis with chronic inflammation 2. Negative for a neoplastic change." Micro was not sent (!) but no organisms seen under histo at least.
showed size now 3.4 cm x 2.1 cm with a central area of cavitation. Because he is a Jehovah's Witness and didn't want surgery (surgery said they would take it out if the patient wanted it), a core needle CT guided bx was done. It showed "1. Reactive fibrosis with chronic inflammation 2. Negative for a neoplastic change." Micro was not sent (!) but no organisms seen under histo at least.



 after
after




 _______
_______


{kind=link}