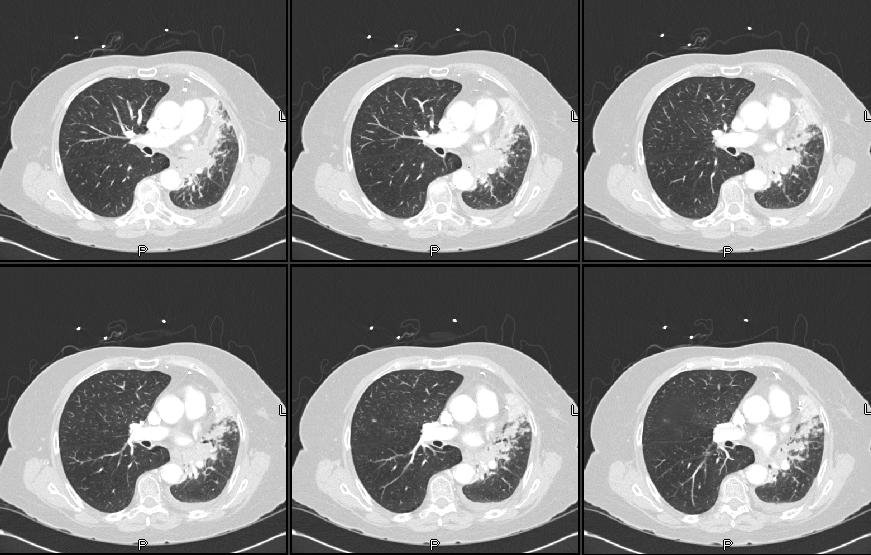
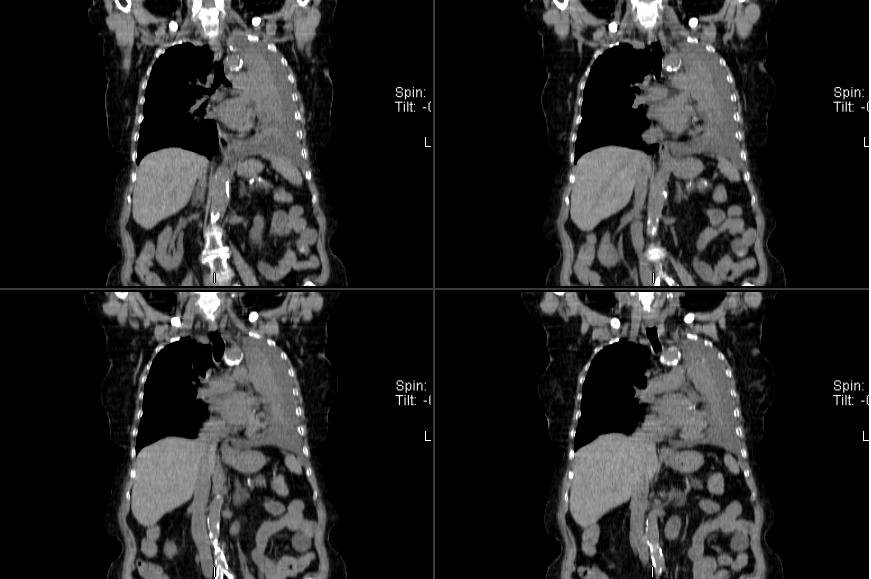
Most of her L lung was collapsed with a smallish effusion. Her effusion was exudative with negative cytology. I did a bronch and she had a NSCLCa occluding her L mainstem bronchus. Her Spiro (with her L lung collapsed) revealed an FEV1~ 800cc.
What would you suggest as the next step?
2 comments - CLICK HERE to read & add your own!:
Well, that there was collapse of the lung due to the cancer makes it a T3 (thus whether the lesion was more than 2cm from the carina is not an added consideration since it's already a T3). The negative effusion is good (thus avoiding a T4 classification). If there are no nodes, this could conceivably still be a stage IIb wich would make it amendable to surgery. The poor FEV1 is likely not to be as bad once the collapse is resolved, therefore this is not necessarily a sign of inoperability. I would get a PET to help determine if there is mediastinal involvement. If, after tht workup we are still left with a stage IIb, I would refer him to CT surg. As far as the FEV1, again, the CT *suggests* that the other lung is relatively free of severe emphysema...
I'd just do the quantitative V/Q scan and, if borderline, a CPET.
Post a Commenttest post a comment