She went to an ID doc, who convinced her the treatment is worse than the disease. So, she opted for no treatment.
She is pretty much asymptomatic since 1/04 (the time of her original CT), but she presented to the ER with hemoptysis (about 5 tbsp, bloody sputum with clots). She was watched in observation overnight and it did not recur.
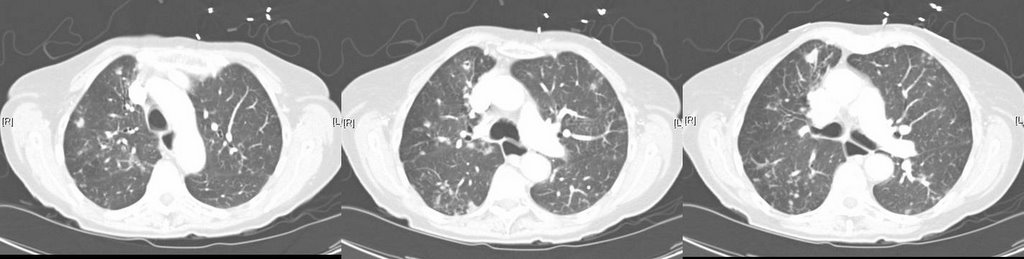
Her repeat CT scan (to rule out PE, of course), showed stable nodules. There were more of them, but the ones visualized 2 years ago are definitively stable.
Would you offer a bronch, or is the CT with bronchiectasis enough to convince you of the diagnosis (she has never before been endoscopically evaluated)?
Would you treat the MAI in this 80 yo, relatively asymptomatic individual?
4 comments - CLICK HERE to read & add your own!:
Pre-existing broniectasis can be a focal point for symptomatic nontuberculous mycobacterial infections such as MAI. This patient has hemoptysis and progression of pulmonary nodules on CT. She has no known liver disease and so I would recommend treatment.
I do think that it would be important to perform further work up (such as bronchoscopy) to exclude neoplastic disease or other causes for the nodules and hemoptysis. Does this patient have a smoking history or other exposure history to increase her risk of cancer?
Great blog BTW!
I would establish the diagnosis of MAI before cosidering treatment. Need more specimens before starting treatment according to the ATS guidelines shown below.
The following criteria apply to symptomatic patients with in-filtrate, nodular or cavitary disease, or a high resolution computed tomography scan that shows multifocal bronchiectasis and/or multiple small nodules.
A. If three sputum/bronchial wash results are available from the previous 12 mo:
1. three positive cultures with negative AFB smear results
or
2. two positive cultures and one positive AFB smear
B. If only one bronchial wash is available:
1. positive culture with a 2+, 3+, or 4+ AFB smear or 2+, 3+, or 4+ growth on solid media
C. If sputum/bronchial wash evaluations are nondiagnostic or another disease cannot be excluded:
1. transbronchial or lung biopsy yielding a NTM
or
2. biopsy showing mycobacterial histopathologic features
(granulomatous inflammation and/or AFB) and one or
more sputums or bronchial washings are positive for an NTM even in low numbers
It's nice to hear from some new people!
I agree with both of the posts above. I think that you should confirm the diagnosis with repeat sputum or with a BAL. Given the prior findings and the pretty typical imaging and the good story, I would feel comfortable with one positive sample (either from sputum or from a BAL).
As to treatment, I think that there is evidence of disease progression and she's had hemoptysis. So, I would offer treatment; if she has adverse effects, than it can be readressed.
I agree with further investigation too. What are her PFTs like? Has she had any physiologic decline. I would not write her off based on age alone. I´ve recently completed MAC Tx for an 83 y/o woman: she used to have copious sputum production and a persistent cough. Her PFTs improved and she has not had a cough in months.
Post a Commenttest post a comment