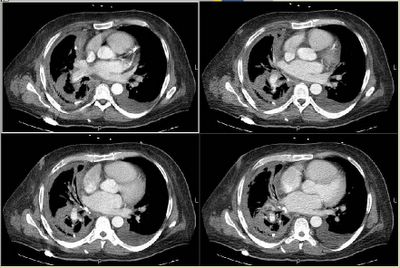
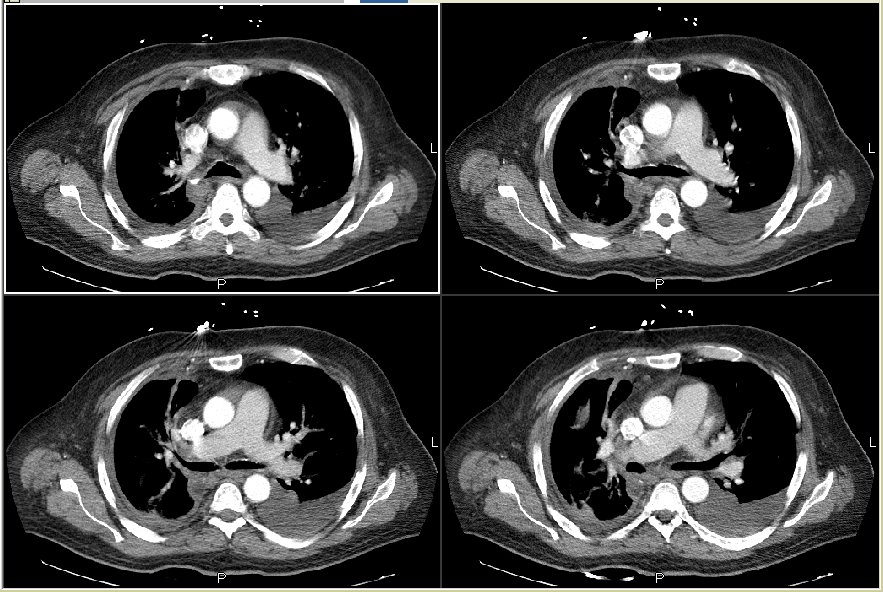
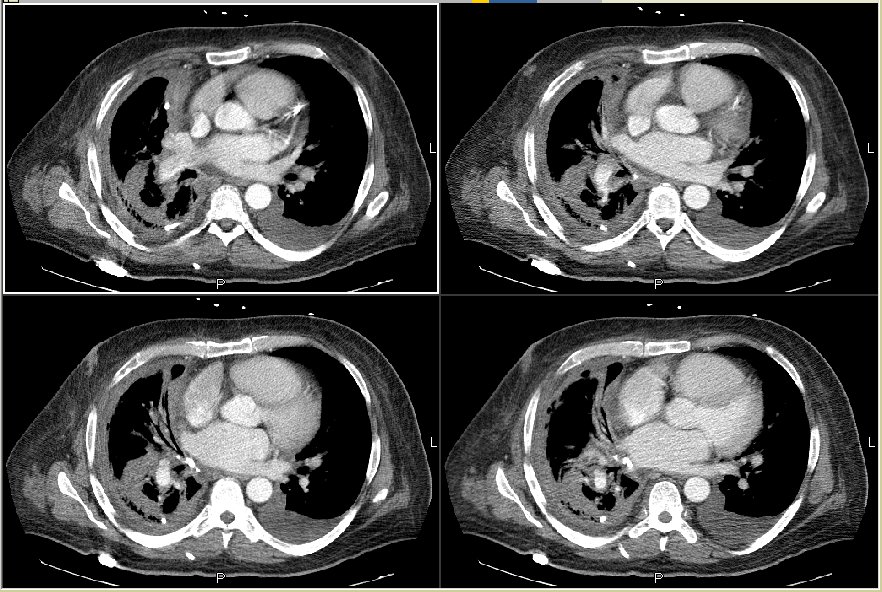
After drainage through the pig-tail catheter he has had marked symptomatic improvement. Pleural fluid cultures grew alpha-hemolytic Strep and Bacteroides fragilis. He is still on Zosyn. As you can see on the scans the major fluid pocket on the left is completely resolved (with thickened pleural and areas of air-space consolidation). He is still going to have surgical decortication but at cardiology's request this will be delayed so he can stay on Plavix/ASA a little longer to prevent hyper-acute stent closure.
I will close this post as mixed flora empyema in the setting of previous chest tube for empyema. Perhaps surgical evaluation during his initial presentation to the OSH would have prevented this progression. If there are any new scans or events I will post them as a separate post at a later time.

3 comments - CLICK HERE to read & add your own!:
In the clinical year in review at ATS in pleural disease, they reviewed an article that noted fibrinolytics in empyema are not valuable.
Maskell NA et al. NEJM 2005; 352: 865-74.
Based upon this, the surgeons are pretty reticent to use fibrinolytics in an empyema and advocate taking the patient to the OR if possible.
I suppose there are those who still favor the use (Y-J?), but it remains to be seen in what subpopulation they are valuable.
We didn't try fibrinolytics either though the perc drainage bought us some time to optimize his cardiac status prior to surgery.
I think the perc drainage approach may be catching on. I've got a patient in the ICU right now--had bilateral traumatic pneumothoraces with chest tubes about two weeks ago. Went home with the tubes out, and 10 days later admitted with severe sepsis requiring pressors. Has a huge empyema (MRSA). Was too unstable for the OR, and we've used a pigtail catheter for the last several days. Have had (surprisingly) good drainage, and she's responded very well. Still febrile, but off of pressors after 24 hours, now mobilizing all the fluid we used to resucitate her. She'll probably go to the OR for decortication tomorrow. So, perc drainage, at least in my case and yours, Carlos, appears to have been a good approach to temporize prior to definitive surgery.
Post a Commenttest post a comment