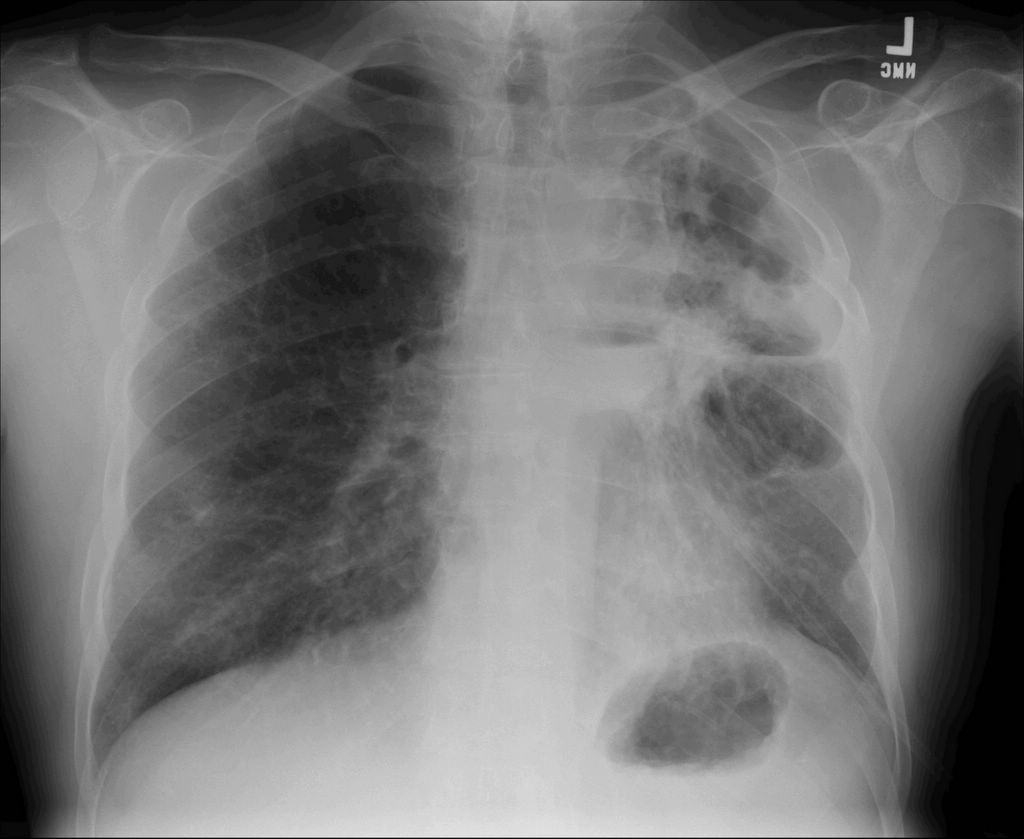
We were consulted on a 55 y/o man with stage IIIB bronchogenic Ca, S/P xRt and chemo. He also has mild COPD and had done fairly well with Chemo/radiation. He is ~8 months since the initial Dx and ~3 months since his last chemo. He now presents with fevers, SOB and cough productive of thick purulent sputum. CxR as below.
He was admitted and started on Ceftazidime. He reports a PCN allergy.
Sputum Cxs have identified a MDR Pseudomonas aeruginosa. It is only sensitive to Piperacilin and aminoglycosides with intermediate sensitivity to Ceftazidime. I re-questioned him about the PCN allergy: in college he had an IM injection of PCN and had an immediate syncopal episode. No rash, no wheezing, no need for hospitalization.
Do you:
continue Ceftaz and add an AG?
Skin test for PCN? (there is a national shortage of purified PCN skin antigen)
Desensitize for PCN?
Document that this is likely not a real PCN allergy and start him on Pip (we only have Pip/Tazo) on formulary?
4 comments - CLICK HERE to read & add your own!:
Is the bug sensitive to imipenem?
If so there is a small cross-reactivity to imipenem. Some sources indicate that if you have a true allergy to PCN, you should not give carbapenems.
That being said, it sounds as if he had a vasovagal response to an IM injection.
After obtaining consent from the patient (i.e. telling him the potential danger of giving pencillin, but with little choice), I would give him imipenem (or whatever carbapenem you have on formulary) with a test dose first.
Alternatively, you could be safe and skin test him for a PCN allergy.
Wouldn't it be nice if someone had decided to test him 20 years sooner given his atypical reaction?
I think all options are reasonable, but here's another thought. Continue the ceftazadime, but escalate the dose. Most intermediate resistance is a laboratory definition. But I believe that you can still achieve bacteriocidal levels even with intermediate resistance.
Otherwise, I'd love to just give the Pip, but I'd cover myself first and either skin test or desensitize. Unfortunately, we all know that any "allergy" that appears in someone's history turns into gospel (even if that "allergy" is constipation due to a narcotic!)
The lab is re-checking the isolate for imipenem (though I have only seen it on two isolates where it was RR to imipenem and SS to Pip).
With the national shortage of PCN derived peptide for skin testing, our pharmacy doesn't have any in stock. I though about increasing the Ceftaz dose. However it tested resistant to Cefepime (with a high MIC) and I was concerned that the Ceftaz intermediate sensitivity might have been a lab artifact.
I will post what I actually did and how things are going once we get some more votes.
Well, while the Imipenem data was pending, I started him on Zosyn. He was already on solu-medrol and as everyone pointed out, he had had an adverse reaction to PCN, not a real allergy.
I did what Mike L suggested: explained the pros and cons and obtained verbal consent and charted it all prior to the first dose of Zosyn. He has tolerated Zosyn well so far.
Post a Commenttest post a comment