Discussion of interesting or befuddling cases related to pulmonary and critical care medicine.
Monday, June 13, 2005
Infiltrates in a 30 year old man
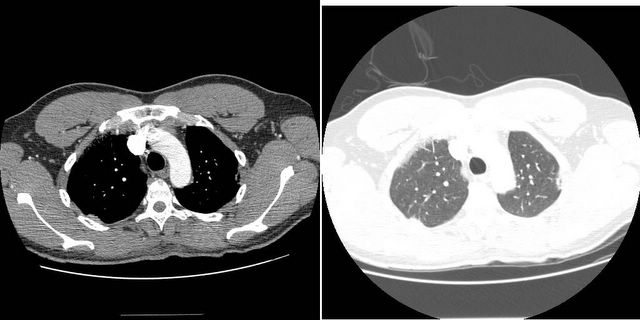
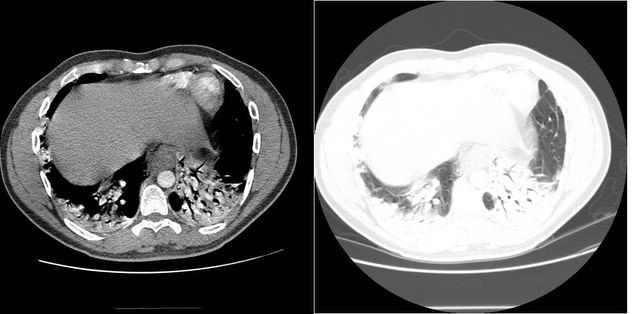
HC wants input on what to do with this patient. 30 year old man no PmHx with 3 months of fevers and malaise. HIV negative. CBC has a normal diff without eos. Based on CT below, bronch attempted but he desatted to the mid 80's so it was aborted.
What would you do next? What do you think this could be?
Unfortunately, he needs a bronchoscopy with a BAL and biopsy. If he needs to be intubated to do it, so be it. I assume that he has had a course of antibiotics that treat typical and atypical pneumonia and he has not improved. Also, is there any chance that this person aspirates (i.e. a drinker?); risk factors for TB? The differential is quite large including infectious, inflammatory, malignant etiologies.
It will be interesting on where most of us fall on how aggressive to be with bronchoscopy.
Before I start the workup, What will you do with the hypoxia..the patient's oxygen sat. is persistantly in the 80's...will you intubate or use bipap or just watch. clinically he is tachypneic and labored. Also, Would you treatr him before you have biopsy result and what will you use? i.e. steroids or Abx
I agree with the differential listed by abetens. The three month history makes bacterial infection unlikely. Age makes carcinoma unlikely, (although this would be a very nice CT for bronchoalveolar cell). BOOP/COP is definitly a possibility.
Given the history of heartburn, I'd add severe reflux with aspiration injury.
It's not too diffuse, so AIP is unlikely, and you havn't given a history of drug use, so right sided endocarditis with septic emboli is unlikely.
If he's in the unit with this CT scan, I'd presume he's on antibiotics to cover CAP. As you're presenting him here, I'm guessing that antibiotics did not make him better. I'd intubate and bronch as suggested by others. If he does ok, you can extubate rapidly. If the bronch with all that others have mentioned is non-diagnostic, I would push for a surgical biopsy. In the meantime, I'd treat for reflux and consider an esophageal pH monitor.
I would vote for the same as suggested above: intubation if he is still so hypoxemic and bronch. Aspiration with mixed flora or atypical agents such as actino could explain this presentation. It seems too focal for IIP's in general. How are his teeth?
His dentitiion are not bad. In my mind it is chronic aspiration vs BOOP. The CT is consistent with both. Because of this, I am contemplating intubation and then directly to VATS (nad have them do a BAL for cell count and micro). The question then becomes, can BOOP and pneumonia (aspiration) be distinguished on biopsy? I would assume that there is less terminal bronchial involvement in the pneumonia). BTW, yes he is being covered for CAP now. A 7 day course of levoflox as outpatient last month did not do anything. A Z-pak for 10 days about 2 weeks ago also did not help. So maybe BOOP is higher on he list now.... BTW, chronic eosinophilic oneumonia is lower given lack of peripheral eos on the CBC, but the bronch cell count will more definitively rule that out.
In addition to aspiration pneumonia, I have seen severe acid aspiration cause a chemical pneumonitis that looked exactly like a pneumonia/BOOP/or BAC. The patient was intubated, the bronch was normal, and everything resolved eventually when he had a Nissan fundiplication. Obviously, the other considerations need to be evaluated first.
BOOP should be easily distinguished from pneumonia on a surgical biopsy by the "tufts" of granulation tissue and the, relative lack of neutrophilic infiltration, and the lack of alveolar involvement (in addition to the involvement of terminal bronchioles that you mentioned).
Thanks for the input; ok I think a VATs with a BAL would be useful then to distinguish BOOPS vs infectious vs chemical aspiration. If former - steroids. If latter - EGD or long-term abx to cover anerobes.
As for no response on Abx, baleeiro is right regarding not ruling out anerobes. I'll let you know what biopsy results are.

10 comments - CLICK HERE to read & add your own!:
Unfortunately, he needs a bronchoscopy with a BAL and biopsy. If he needs to be intubated to do it, so be it.
I assume that he has had a course of antibiotics that treat typical and atypical pneumonia and he has not improved. Also, is there any chance that this person aspirates (i.e. a drinker?); risk factors for TB?
The differential is quite large including infectious, inflammatory, malignant etiologies.
It will be interesting on where most of us fall on how aggressive to be with bronchoscopy.
Before I start the workup, What will you do with the hypoxia..the patient's oxygen sat. is persistantly in the 80's...will you intubate or use bipap or just watch. clinically he is tachypneic and labored.
Also, Would you treatr him before you have biopsy result and what will you use? i.e. steroids or Abx
History update:
Heartburn for 3 years. Occassional nocturnal heartbearn. Hemoglobin 12.
EGD: Grade II esophagitis, 3 cm hiatal hernia; duodenitis. No ulcers.
NOW what would you do in with him? He is in the unit satting in the low 90's with the CT shown above.
I agree with the differential listed by abetens. The three month history makes bacterial infection unlikely. Age makes carcinoma unlikely, (although this would be a very nice CT for bronchoalveolar cell). BOOP/COP is definitly a possibility.
Given the history of heartburn, I'd add severe reflux with aspiration injury.
It's not too diffuse, so AIP is unlikely, and you havn't given a history of drug use, so right sided endocarditis with septic emboli is unlikely.
If he's in the unit with this CT scan, I'd presume he's on antibiotics to cover CAP. As you're presenting him here, I'm guessing that antibiotics did not make him better. I'd intubate and bronch as suggested by others. If he does ok, you can extubate rapidly. If the bronch with all that others have mentioned is non-diagnostic, I would push for a surgical biopsy. In the meantime, I'd treat for reflux and consider an esophageal pH monitor.
I would vote for the same as suggested above: intubation if he is still so hypoxemic and bronch. Aspiration with mixed flora or atypical agents such as actino could explain this presentation. It seems too focal for IIP's in general. How are his teeth?
His dentitiion are not bad. In my mind it is chronic aspiration vs BOOP. The CT is consistent with both. Because of this, I am contemplating intubation and then directly to VATS (nad have them do a BAL for cell count and micro). The question then becomes, can BOOP and pneumonia (aspiration) be distinguished on biopsy? I would assume that there is less terminal bronchial involvement in the pneumonia).
BTW, yes he is being covered for CAP now. A 7 day course of levoflox as outpatient last month did not do anything. A Z-pak for 10 days about 2 weeks ago also did not help. So maybe BOOP is higher on he list now....
BTW, chronic eosinophilic oneumonia is lower given lack of peripheral eos on the CBC, but the bronch cell count will more definitively rule that out.
I wouldn't disregard infection based on the lack of response to ABTx: both levaquin and azithro would not cover aspiration with mixed flora very well.
In addition to aspiration pneumonia, I have seen severe acid aspiration cause a chemical pneumonitis that looked exactly like a pneumonia/BOOP/or BAC. The patient was intubated, the bronch was normal, and everything resolved eventually when he had a Nissan fundiplication. Obviously, the other considerations need to be evaluated first.
BOOP should be easily distinguished from pneumonia on a surgical biopsy by the "tufts" of granulation tissue and the, relative lack of neutrophilic infiltration, and the lack of alveolar involvement (in addition to the involvement of terminal bronchioles that you mentioned).
Thanks for the input; ok I think a VATs with a BAL would be useful then to distinguish BOOPS vs infectious vs chemical aspiration. If former - steroids. If latter - EGD or long-term abx to cover anerobes.
As for no response on Abx, baleeiro is right regarding not ruling out anerobes.
I'll let you know what biopsy results are.
addendum - not EGD - he's already had this. Sorry.
Post a Commenttest post a comment