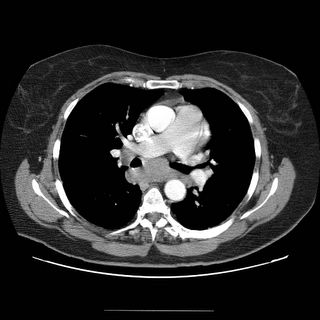
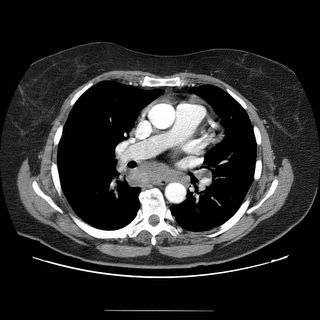
I saw in clinic a 62-year-old woman with no past medical history who first developed mild dyspnea on exertion about two months ago. She had just retired from her job working in a supermarket (lifting and moving boxes in the warehouse section). After walking up a flight of stairs, she became severely short of breath. She came to the ER, where a VQ scan was high probability. A pe-protocol CT was also done and it confirmed bilateral filling defects in a number of pulmonary arteries. She was started on Coumadin for this. Now she is left with fatigue and dyspnea on exertion. No weight loss or anorexia. Here’s what the CT showed (click to enlarge them).

SOCIAL HISTORY: The patient is a lifelong nonsmoker.
PHYSICAL EXAMINATION: The patient is an obese white woman Weight: 277 pounds. Rest of exam unremarkable.
Spirometry was normal.
It always happens to the nice ones (or the ones that JUST retired).
Anyway, what are your thoughts?


11 comments - CLICK HERE to read & add your own!:
I will try to start the discussion focusing on some of the CT findings. I will assume from your description that there was clot throughout on other images in addition . There is very little flow suggesting a submassive occlusion. Is that the original CT scan?
In addition to the poor perfusion, I am impressed by the mediastinal adenopathy. It seems pretty full in the subcarinal space and I can see some more on the right hilum. erhaps she has an occult malignancy, lymphoma or CLL would fit the bill with acquired thrombophilia and PE.
The questions now will focus on treatment of the PE/PHtn and w/up of malignancy/thrombophilia, unless you tell me I am reading too much on that mediastinum.
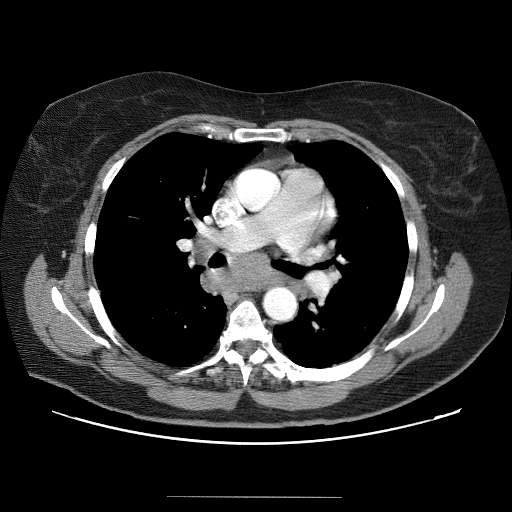
You are not reading too much into it. There is definitely lots of adenopathy. The lung slice I provided was to show that there is also a small nodule.
So she had pulmonary embolus, adenopathy and a small nodule. This isnt a trick question in terms of zebras.
Any second-hand smoke exposure on the Hx?
No second hand smoke exposure. The radiologist who read it confirmed the filling defects for the embolus but to quote him regarding the adenopathy, "there is adenopathy in the peritracheal, pre-vascular, AP window,subcarinal, aortocaval and paraesophageal. The largest lymph node is subcarinal."
And regarding that lung nodule I showed you, "Multiple nodules in the right and left lung: metastastic disease is highly suspected. A primary lung focus is not appreciated.
How certain are you that all of the mediastinal "fullness" is adenopathy and not, at least partially, a thickened esophagus? My monitor has pretty lousy resolution and I cannot differentiate.
Oh, and is there anything in her breasts (i.e. a mammogram) or in her kidneys on the CT of the chest?
I think you could probably make a diagnosis with a transbronchial needle aspiration (Wang) if it is carcinoma; for lymphoma, you would need a mediastinoscopy. However, you may want your GI collegues to run her esophagus and colon first.
Good point Mike L...Yes the the esophagus is abutting the nodes. Therefore when the wang came back as just a bunch of epithelial cells, I had her go for esophogeal USG-guided biopsy. The cytology on that procedure showed not much, just "[...] within blood clot are some clustered cells suggesting granuloma formation. Special stains for pathologic bacteria (AFB and Grocott) are each interpreted as negative, but are considered to be of low sensitivity"
There is also a possibility that the "clots" are actually vascular extension of a primary tumor elsewhere. Renal cell likes to invade the IVC and to embolize.
She might be more fortunate and have a systemic granulomatous infection. Hysto Ag and a PPD may help.
Given the differential here, I think histo/blasto etc. could be considered extremely fortunate! I agree with all that has been said--at this point I think a mediastinoscopy is necessary, although not much fun given her ongoing need for anticoagulation.
I think baleeiro's point about an intravascular tumor is an interesting one. There was an amazing "Images in medicine" in NEJM a few months (April 14, Vol 352 #15) ago showing a case of that-check it out...
http://content.nejm.org/content/vol352/issue15/
Horowitz's rec was what I did - mediastinoscopy, because of the nondiagnostic USG. The results of path from that:
"lymph node architecture is effaced by multiple non-caseating granulomas composed of multinucleated giant cells and epithelioid histiocytes." No cancer. Special stains for fungal and TB negative.
Anyway, to wrap this us, there is a 60 y/o caucasian woman who presents with pulm embolus and adenopathy - this really seems to be cancer. The age group and race may throw one off - but in the end it turns out to be sarcoid. Interesting eh? Ok on to baleeiro's case...
Post a Commenttest post a comment