This is a 62 y/o man with mild COPD (FEV1~75%) who was being worked up for mitral valve insufficiency. A CxR revealed the following abnormalities and he was referred to us:

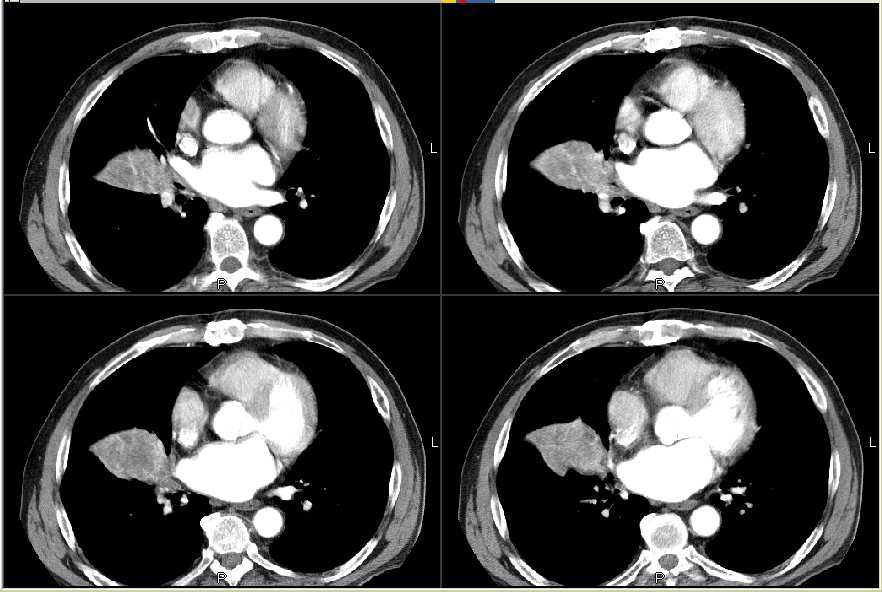
He had quit smoking in 1989 and on his first visit he had some symptoms of a respiratory tract infection (F/C and a productive cough). Those improved with ABTx but his CxR was still abnormal and a CT scan was performed:


I bronch'ed him and other than an acute tracheobronchitis, he had widely patent airways and no endobronchial lesions. TBBx from the area were non-Dx.
Clinically he improved and he did not want anything more invasive at that time so we waited a couple months, added an ICS and ABTx and repeated a CT scan:
Since he was being evaluated for possible repair of his mitral valve, his CT surgeon asked us to re-bronch him. The tracheobronchitis was gone, airways were open and TBBx from the same area, BAL and washings were non-Dx.
What would you do next?
1 comments - CLICK HERE to read & add your own!:
That's very intersting. Fromt the cuts of the CT scan, it definitely looks like there is an obstructed bronchus on the right, with post-obstructive atalectasis. However, it is atypical that the post-obstructive region doesn't extend to the pleura. Additionally, there are no air-bronchograms in the consolidated area, similarly suggesting a complete occlusion. But, no obstruction was seen on two different bronchoscopies.
I don't see any vessels leading into the densely consolidated area, although a sequestration is possible. Are there any prior chest xrays for comparison?
It's interesting that he did have symptoms of infection initially. This would be an atypical presentation of BOOP. Bronchoalveolar cell carcinoma can easily look like this, but between the two bronchoscopies I'd expect some abnormal cell on the transbronchs.
Could this be related to his mitral valve disease? I don't have all of the cuts, and I don't see the pulmonary outflow tract or clear pulmonary arteries. The pulmonary veins and (I presume) the left atrium seem a bit prominant, but I find it hard to believe that enlarged pulmonary veins can compress/occlude a segmental bronchus. It would be helpful to see all of the cuts so that I could track the anatomy better...
Finally, it does seem to "respect" the fissure, so I wonder if this is a loculated fluid collection in the fissure--a "pseudotumor" per se.
At this point, malignancy remains my primary concern. I'd do a PET for staging, and unless the PET is definitively positive elsewhere, I'd recommend resection. His FEV1 is 75% predicted, so he should tolerate a lobectomy well.
Post a Commenttest post a comment