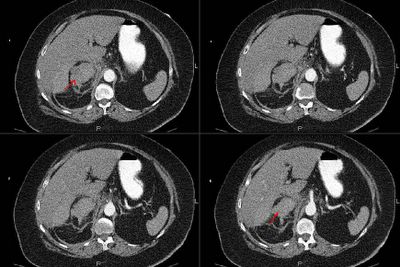
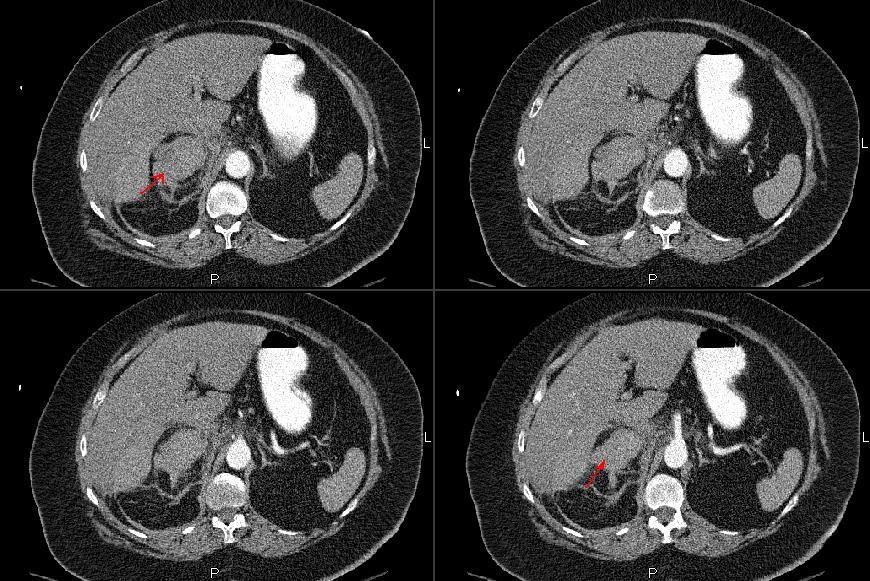
I will make the history brief. An obese 70 y/o woman with a known adrenal adenoma presented with R flank pain with referred R shoulder pain, nausea and vomiting. She had the following CT scan:
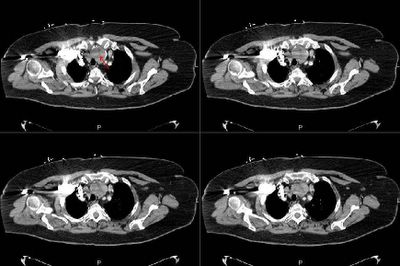
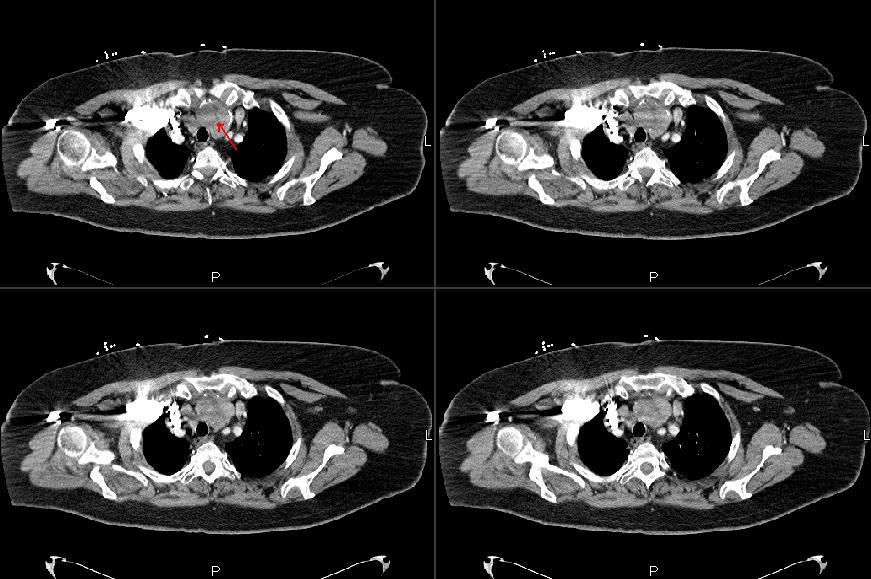
She was hospitalized and last night developed dyspnea and CP and the following CT images were obtained and we were consulted.
What are the highlighted findings and what would you do next?

3 comments - CLICK HERE to read & add your own!:
Ok, I will take a shot at this one. I will not list ANY worms, parasites or intracellular organisms in my differential.
It seems as if the top CT has a mass in the right adrenal. It would be nice to actually be able to trace it to the kidney to confirm that is truly what it is. Without contrast it is hard to tell if it is truly an adenoma or potentially more "dangerous" than that.
The CT of the chest shows an anterior mediastinal mass just posterior to the sternum. This is the 4T's of teratoma, thyroid, thymus and tlymphoma (that means terrible lymphoma). Is it safe to presume that the lung windows are normal?
The contrast windows show a pulmonary embolus in the left pulmonary artery (both upper and lower lobe branches).
What to do?
Well, I would send off a TSH, T4, AFP, B-HCG, and cortisol levels to get some serologic markers. Most oncologists want about 15 others, but they can be sent at a later time.
Oh, and I would start her on heparin.
I think I would biopsy the ant mediastinal lesion first unless the radiologist told me that the adrenal lesion is clearly malignant.
And, no, Kala Azar is not in my differential.
Sorry, sorry, sorry...
Well, to put the mediastinal mass, the embolus and the adrenal mass together, you would have to come up with something with high metastatic potential *and* that is associated with a hypercoagulable state. A thymoma is rarely metastatic. A thymic cancer can metastasize, but there should be some regional LN involvement as well.
I wouldn't expect teratomas to spread to distant sites without evidence of invasion to adjacent structures.
Alternatively, Small cell cancer would fit; adenocarcinoma predisposes to prothrombotic state and metastasizes to the adrenal, but would not explain the anterior mediastinal mass. Of course the adrenal finding may be benign but if it was, you probably wouldn't have posted it.
The other thought; let's say this is hodgkin's lymphoma (the mediastinal mass) and the lesion on abd CT represented something with the kidney. We know that hodgkins predisposes to nephrotic syndrome via minimal change disease which in turn would give the patient an increased risk of hypercoagulationa nd the embolus seen here....
Very cool DDx and suggestions. I will post some preliminary answers because we are going out of town (it's Sophia's first B-day).
That is indeed a large thyroid mass on the second pic with B/L PEs on the third.
The adrenal mass doesn't show it very well but there is a bleed in it: the original pain was a hemorrheg into the mass with some retroperitonial blood. The problem was then the bleed with a new PE...
She had an IVC filter placed yesterday and is being watched in the ICU. I will post a follow up as the case develops.
Post a Commenttest post a comment