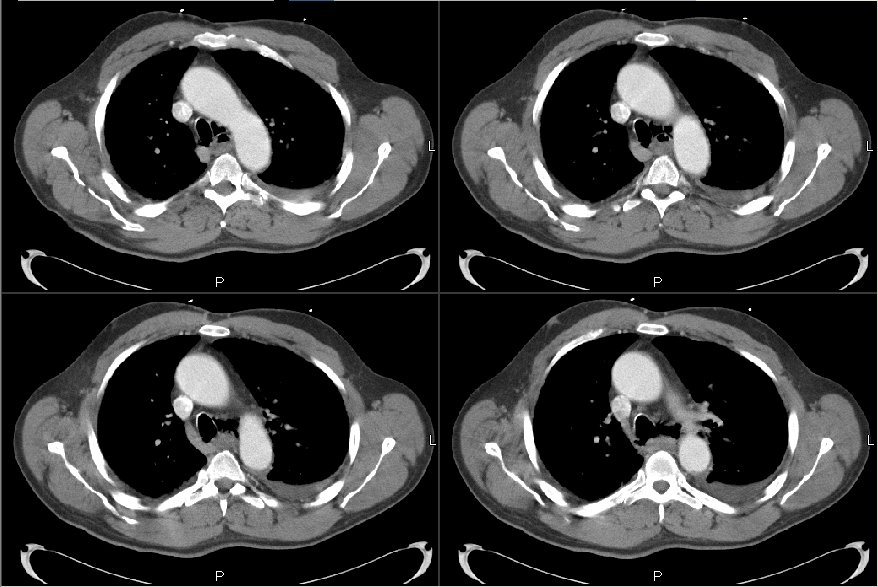
On the first few cuts, it looks like the esophagus and the tracheo-bronchial tree are in communication, but this may be technique. In either case, there looks like some air around the great vessels and the left pericardium, along with a left basilar consolidation. The mediastinal soft tissue looks shaggy and wide.
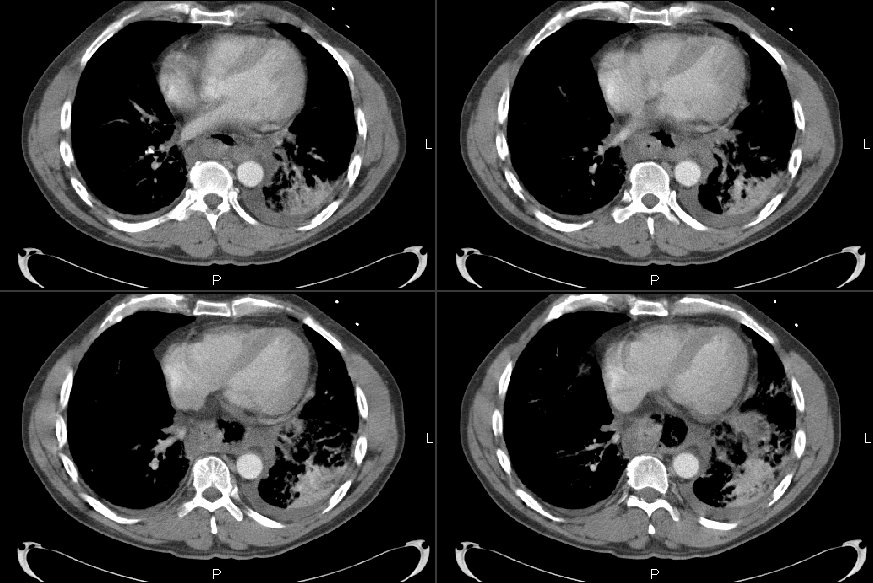
The CT confirms the effusions (which I didnt see on the plain film), which likely represents the gastric contents as a result of an esophogeal perforation. I can't see the actualy perf on the CT but I would guess that it is consistent with horowitz's thought of Boerhaave's. I agree with calling thoracic surgery (and the antibiotic coverage).
The patient had Boerhaave's indeed. The CT shows the esophageal rupture and pleural fluid with aspiration pneumonitis on the left (very typical). He was started on ABTx and taken to surgery. His cultures from surgery and the pleural fluid grew a smorgasbord of bacteria including Prevotella and Bacteroides. He did remarkably well and was eventually D/C'ed home. I just saw him in the office last week and he is back to baseline, has quit smoking and has but a mild obstructive defect (FEV1~74%). Final diagnosis: Boerhaave's with pneumonia, empyema and pneumomediastinum.

3 comments - CLICK HERE to read & add your own!:
On the first few cuts, it looks like the esophagus and the tracheo-bronchial tree are in communication, but this may be technique. In either case, there looks like some air around the great vessels and the left pericardium, along with a left basilar consolidation. The mediastinal soft tissue looks shaggy and wide.
I'd get a thoracic surgeon involved quickly.
The CT confirms the effusions (which I didnt see on the plain film), which likely represents the gastric contents as a result of an esophogeal perforation. I can't see the actualy perf on the CT but I would guess that it is consistent with horowitz's thought of Boerhaave's. I agree with calling thoracic surgery (and the antibiotic coverage).
The patient had Boerhaave's indeed. The CT shows the esophageal rupture and pleural fluid with aspiration pneumonitis on the left (very typical). He was started on ABTx and taken to surgery. His cultures from surgery and the pleural fluid grew a smorgasbord of bacteria including Prevotella and Bacteroides. He did remarkably well and was eventually D/C'ed home. I just saw him in the office last week and he is back to baseline, has quit smoking and has but a mild obstructive defect (FEV1~74%).
Final diagnosis: Boerhaave's with pneumonia, empyema and pneumomediastinum.
Post a Commenttest post a comment