70 year old previous 30+ pack year smoker with hypertension and GERD who presented with flank pain and found to have a UTI/pyelonephritis and treated successfully with Cipro. No fevers chills diaphoresis or cough. But he did admit to a 30 pound weight loss without anorexia over about 6 months. A routine CXR showed a nodule:
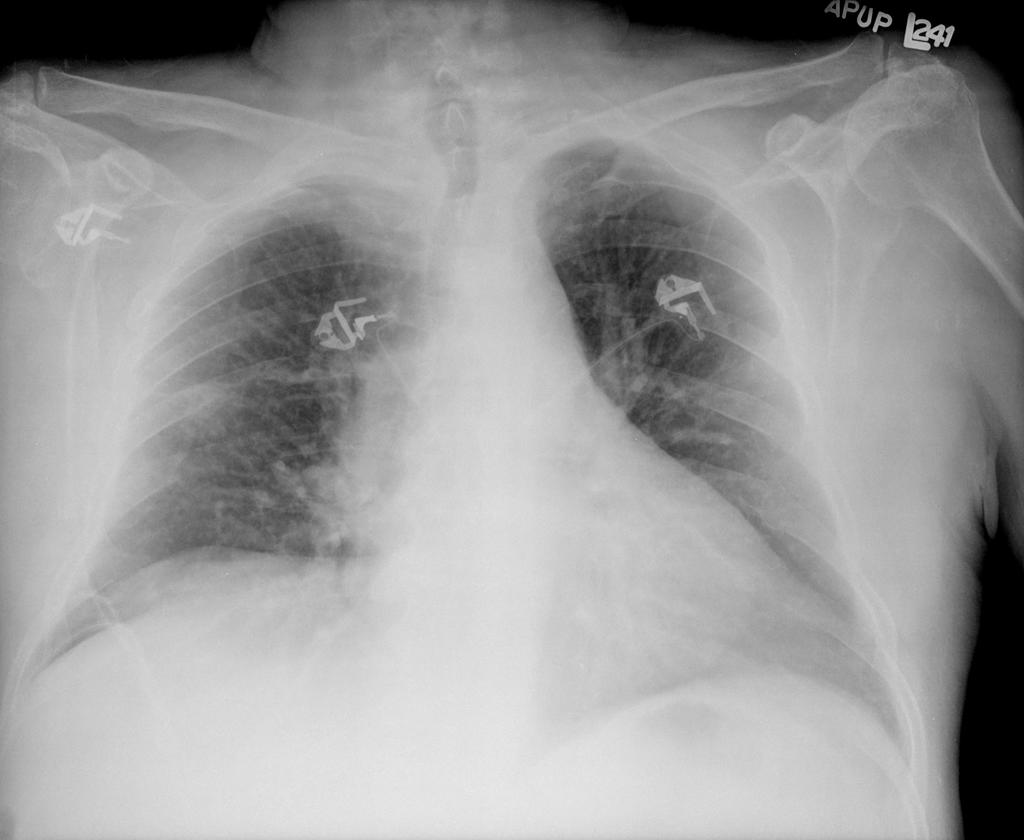 . A CT shown here
. A CT shown here  confirms that. In follow up clinic a month later the CXR looked better:
confirms that. In follow up clinic a month later the CXR looked better: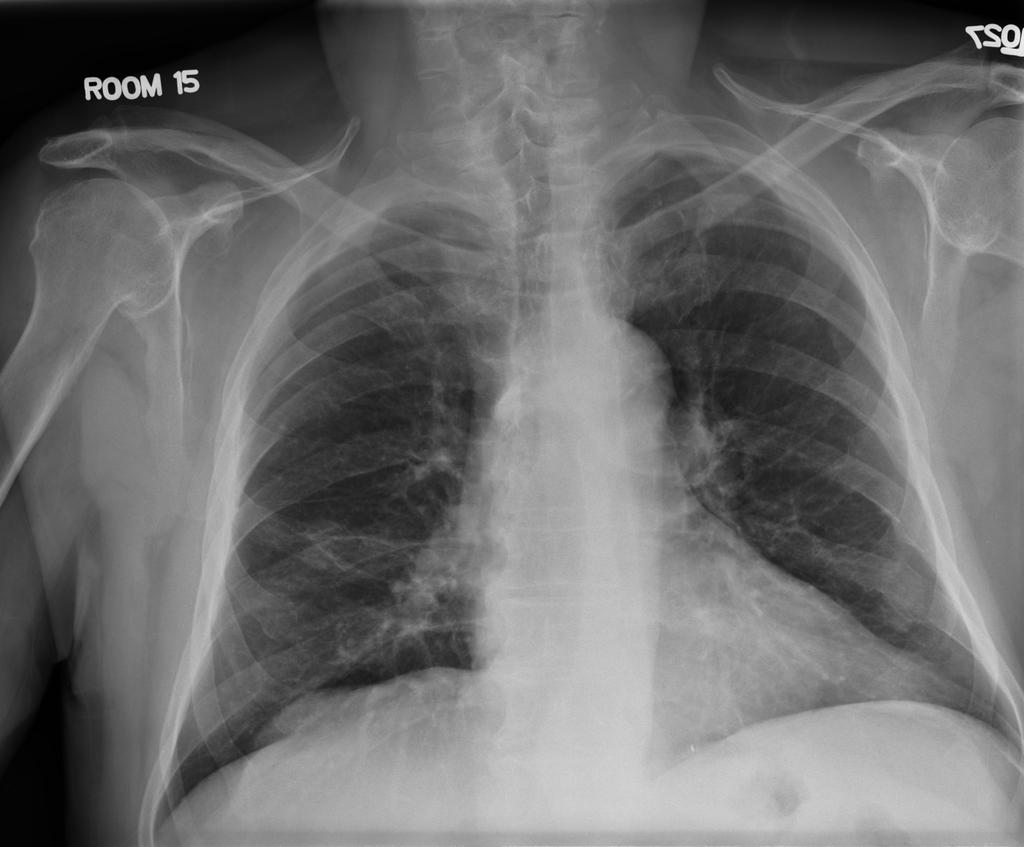 but a CT a month later looked like this:
but a CT a month later looked like this: . What would you do next?
. What would you do next?After you read the comments, the histology (and answer) can be found here.
7 comments - CLICK HERE to read & add your own!:
Was there any mediastinal lymphadenopathy? also, any risk factors for tuberculosis? previous PPD?
While malignancy is abviously the major concern here in this heavy smoker with this cavitary lung lesion (not so typical for squamous ca to be that peripheral), I would still like to rule out an underlying infection, mainly tuberculosis especially with the rather rapid development of that ground glass like opacity around it (as if it was starting to develop on the initial film). Both would give weight loss. I would get PPD and obtain sputum samples, and if he does not make any sputum, bronchoscopy with BAL (send it for cytology besides infectious stuff....)
Mendez, shouldn't you be changing a diaper?
Anyway, I share his concern about malignancy in this cavitary appearing lesion. However, I suppose TB, fungus, WG or even an anaerobic infection in his lung would be plausible.
Before starting any procedures on this guy, I would get a PPD and an ANCA. If the PPD is positive, sputum cultures for AFB should follow.
How healthy is this guy otherwise? If he has good PFT's and performance status (and the above are non-diagnostic/negative), I would have the surgeons wedge it out and convert to a lobectomy if it is cancer via the path on the OR.
This all presumes that the mediastinum, liver and adrenals are negative per krayem's earlier comment.
PPD negative. His lung function is good. An ANCA was not done I dont think. Oh, and the mediastinum was fine. The decision was to cut it out. A PET was not done since it will light up with every single thing on the differential. I am awaiting the pathologist to email me the JPG of the slide. Any other thoughts while we're waiting?
I agree with most of the discussion, and would have favored resection (as was done).
One point to raise, as devil's advocate here: why place a PPD on this patient. A positive PPD doesn't mean it's not cancer, and a negative PPD (as is the case here), does not exclude MTB infection here. For that reason, a bronch with BAL for culture would have been quite reasonable prior to surgery, but I would not have wanted to wait the 6 weeks for negative cultures...
My point is: the PPD is a screening test for LTBI. It has no role in diagnosis or exclusion of active TB in a patient with a radiographic lesion.
And, BTW, thanks for email Mendez! Congrats!
A PPD in this case would alert you to him having been exposed to MTB in the past. If it was positive, I would have bronched him first to r/o active disease. To me, a lack of AFB on that smear would be indicative of non-contageous (?sp) TB.
You are right to say that the nodule would probably need to come out anyway down the line. However, I would try 4 drugs for about 6 weeks and repeat the scan before taking him to the OR for definitive therapy. If the nodule was cancer, it should not grow to "unresectable" status in that time, but might shrink if it were TB.
I think the surgeons might be irritated if they took out active TB in the OR (and exposed the entire OR staff to active TB) when a bronch with a BAL might make the diagnosis first.
True, true, and unrelated. A positive PPD would indicate past exposure, and nothing more. A negative PPD does not mean that it is not MTB. If this cavitary lesion were MTB, I would expect the BAL smear to be positive, or the culture to be positive rapidly, as cavitary leasions with MTB should have a large burden of microorganisms, and would then agree with treating first.
So, I would bronch first anyway. If the smear was negative, I'd move for resection. If the smear was positive or if after a few weeks the culture was positive, I would treat. If it is smear negative and culture negative after a few weeks, than I'd move for resection. Either way, the PPD does not affect my management in this patient.
See histo here: http://pulmonaryroundtable.blogspot.com/2005/08/follow-up-to-patient-with-solitary.html
Post a Commenttest post a comment