PAST MEDICAL HISTORY: Obstructive jaundice secondary to gallstones; COPD per his PCP's records.
SOCIAL HISTORY: Smoking history: 20 pack years; he quit 15 years ago.
Alcohol use: The patient admits to 6 to 7 beers per week for approximately 60 years.
He denies IV or street drug use. He was exposed to asbestos for approximately 7 months as he was working in a factory in which the asbestos was being removed. No travel.
PE: Vitals: Heart rate 76, resps 18. BP 136/76. Saturation: 96% on Room Air. Neck: No JVD. Heart: Normal. Lungs: clear throughout all fields, however, decreased BS in all fields. Extremities: Fingernails positive for clubbing. Pitting edema noted in the lower extremities.
Labs: Sodium 142, potassium 4.3, chloride 110, bicarb 23, BUN 6, creatinine 1.0, glucose 98, calcium 8.2, phosphorus 2.7, albumin 2.3, total protein 5.0, alk phos 151, AST 26, ALT 38, total bili 3.5, direct bili 1.8.
white blood cells 8.6, H and H 9.4, and 29.7 platelets 771.
RADIOGRAPHS:

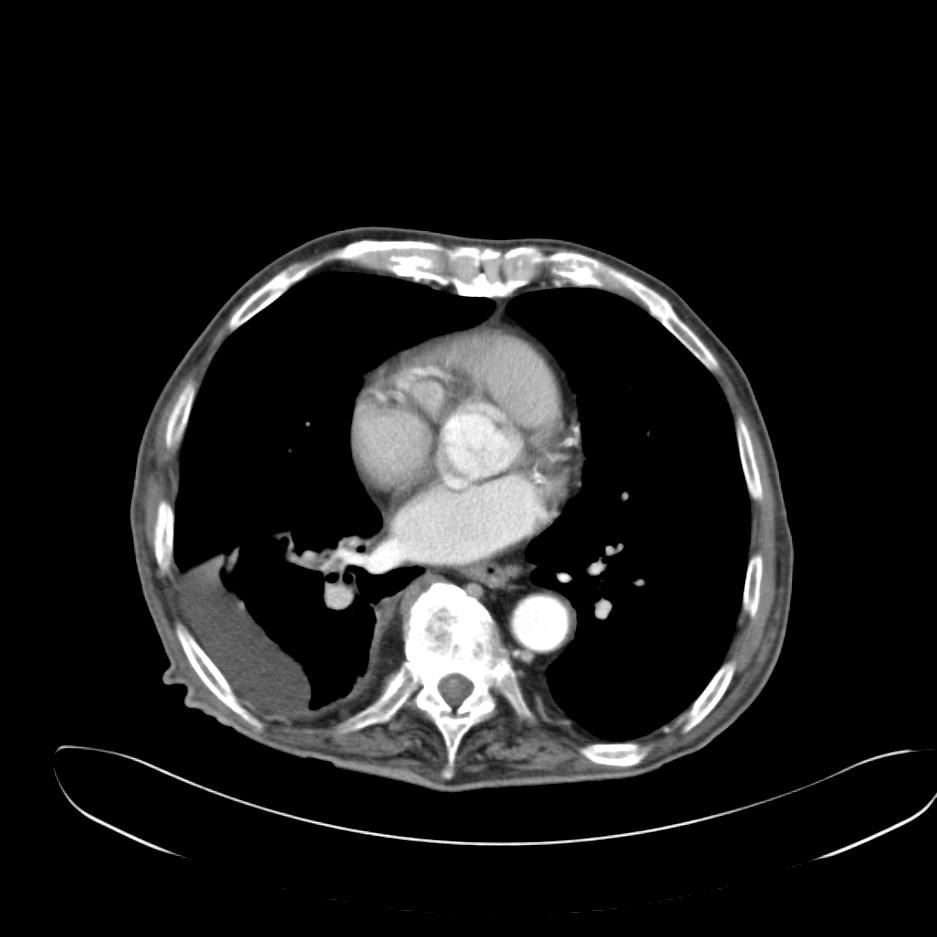
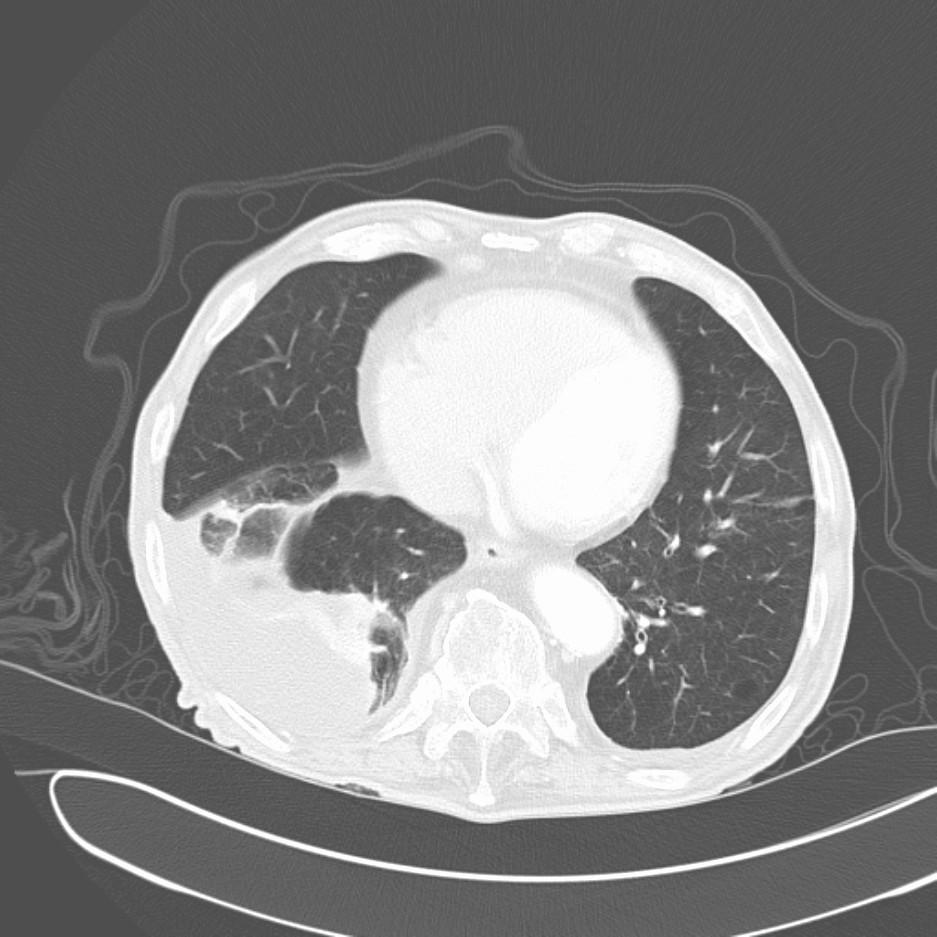
How would you proceed? What tests would you want next?
8 comments - CLICK HERE to read & add your own!:
Were there any immediate complications after the ERCP? The fact that the effusion seems to involve the pleura abutting the mediastinum and pericardium, I would worry about mesothelioma. Was the 7-mos of asbestos exposure a long time ago?
Needs thoracentesis obviously.
That's a pretty small effusion to be causing so much dyspnea. An ultrasound guided tap may be helpful, the the history doesn't really suggest infection. Mesothelioma also doesn't seem likely here.
I may be really overcalling this, but that right PA looks like it narrows pretty quickly. I'd be concerned about a PE here, and would consider a PE protocol CT and lower extremity dopplars to start with.
I agree with smapling the effusion but it seems too small for the dyspnea (as JCH pointed out). The pleura does not seem very thick or calcified but his could be BAPE if the asbestos exposure was significant and no CxR was done prior to the ERCP.
If he has a pre-ERCP CxR (does he?) and the effusion is new, PE would be a concern or sympathetic pleuritis/pleurodynia with inflammation from the inflammed RUQ would be possible (the effusion is on the R).
The ERCP was supposedly uneventful.
So, I tapped him (with marking from ultrasound).
Total Pleural fluid 1.3 L
pH = 7.37; Glucose: 105, LDH: 43, Protein 2.5; Albumin 1.3
Serum Values: LDH: 130, Protein 5.0; Albumin 2.3
Gram stain: No organisms
RBC: 54 WBC: 123 (2 N, 88 L, 10 M)
Cytology:
EXTENSIVE YELLOW-GREEN PIGMENT WITHIN BACKGROUND AND HISTIOCYTES (BILE?) --- NO NEOPLASTIC CELLS PRESENT
I agreed the the dyspnea-out-of-proportion to his pleural effusion size comments?
What would you do next
Do a HIDA scan and look for signal in the pleural space???
He became symptomatically much better after the pleural effusion was drained. I suppose there was some diaphragmatic dysfct associated with its location.
As for the bile, there is a whole literature related to pancreatico-pleural fistulae, but I could not find anything about loculated pleural effusions after ERCP for biliary stone disease. Besides, his pleural fluid did not reaccumulate after the tap.
I did some spirometry on this guy and he had an FEV1 of 34% predicted with a relatively preserved FVC.
I started some oral corticosteroids, advair and PRN combivent and will have him f/u with me in clinic.
Anecdotally, I've had a similar case lately: the guy had a cholecystectomy (rather than ERCP) and had some gallstone spillage in the RUQ. He went home and returned with terrible R chest pain, a moderately sized exudative effusion and some hepatic capsular inflammation. We drained the effusion, gave him some steroids and all went away...
We would be very pleased to have a link on your blog. Thank you for your kind comments and keep checking our blog.
Post a Commenttest post a comment