A 74y/o woman was transferred to our institution for her persistent lung abscess. Briefly, she was an otherwise healthy woman until about 5 years ago, when she was diagnosed with a distal esophageal carcinoma, for which she underwent resection with an esophageal pull through and subsequent radiation therapy. Obviously, she did pretty well. About 6 months prior to her current presentation, a LUL nodule was found, and she underwent a left-upper segmentectomy. Following that, she has been seen for a persistent left pleural and pericardial effusions. The etiology of these remained unclear, and she was told it was a "Dressler's type of syndrome."
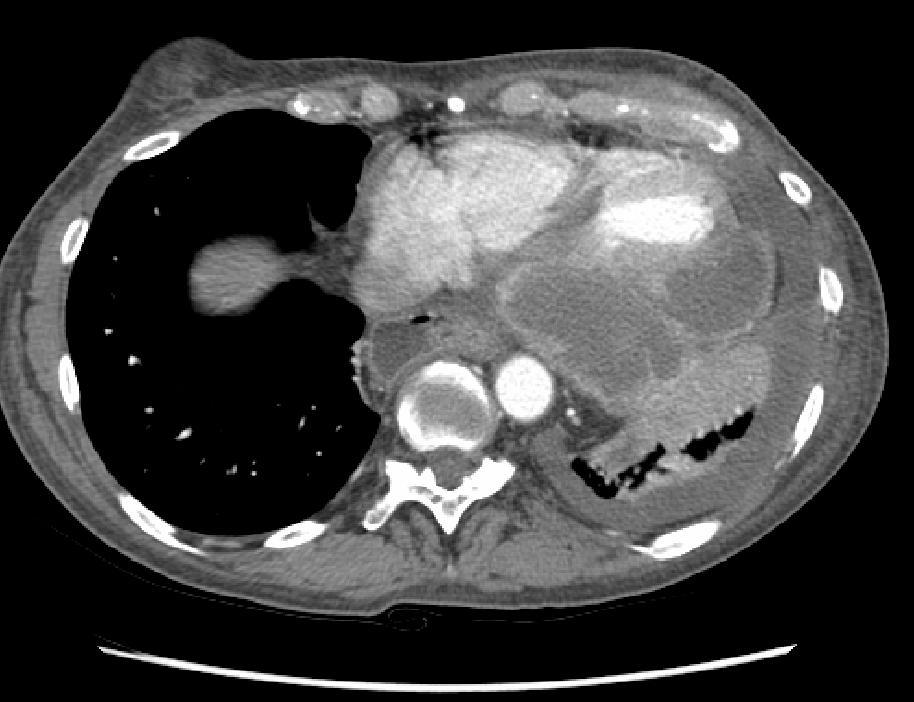
Over a few weeks prior to her transfer, she has developed progressive shortness of breath. No fevers/chills/sweats. No cough or sputum production. No complaints of pain anywhere. She was admitted to another hospital, a chest CT was obtained, and she was transferred to our institution for further management of her lung abscess. Here is a cut from the CT scan done at our institution:

Any comments on the CT scan? Differential diagnosis? Diagnostic studies?
Answer in the comment section below.
17 comments - CLICK HERE to read & add your own!:
It looks as if this patient is in some trouble. That abscess is huge and given the pleural thickening that does not seem to "house" your abscess, it seems as if it is intraparenchymal. The abscess seems to cross the midline and sit in the right perispinal area as well. The cut you provided does not outline the pericardium well, so we do not get a good look at it.
Again, I am pretty lousy at reading films and I would gladly yield to others who are better.
The diff dx is large and ranges from anaerobes from the mouth with an aspiration event to a small GI-pulmonary fistula that developed when they did the lung surgery.. I also wonder if she had an infected pleural space at one point that seeded the parenchyma.
I would do the following:
1. Bronchoscopy to better define her airways. I would try to BAL the LLL to get an organism (if pus was not visible on the bronch).
2. An UGI contrast study with gastrograffin to see if the pulmonary tree lights up with instillation of contrast
3. Antibiotics
Wow!
This is very impressive. The abcess is quite complex and, as Mike pointed out, seems intra-parenchymal (we can see a separate pleural effusion). I can't quite make out whether the pocket of fluid on the other side is part of the pull-through with mediastinal shift or if there is a smaller R abcess. The anterior chest wall also looks funny (you did mention radiation, right?). Aspiration or problems with the pull-through are an obvious concern. I will add Actino and Nocardia as causes of poor resolution.
Is she a smoker? Was the esophageal Ca an adeno or a Squam (different risk factors that may help us).
Granted, this is only one cut, but I assure you that this is quite representative. As I don't want things to get off track here, I'm going to refocus a bit. When I was first shown this film, my thoughts were "wow, that doesn't look like any lung abscess I've ever seen."
Now, I'm going focus you on what Lazar pointed out--it does not outline the pericardium well--and ask a question: is this (whatever you might call it) actually in the lung?
She is a former extensive smoker, but has had pretty unremarkable PFT's. I believe that her prior esophageal carcinoma was squamous, and her resected lung carcinoma was a separate/unrelated primary non-small cell.
The patient was started on Unasyn and Clindamycin pending further work-up.
elevated left diaphragm, oral contrast seen in the gastric fundus, tubular liquid density is probably colon (status post-op).
definitely not lung abscess.
There is a sliver of lung with consolidation posterior to the abcess so it may not be in the parenchyma. If this is arising from the pericardium it is even more impressive.
It seems so complex that a recurrent or a new carcinoma with necrosis and secondary infection is also a concern.
The contrast seen anteriorly was IV contrast; no oral contrast was given for this CT scan.
In fact, neither I, nor two radiologists was able to determine if this collection was in the lung parenchyma or involving the pericardium...
I'm going to go out on a limb here and say that this represents something with the GI; just to the right of the heart - is that oral contrast? And the abuttment with the pericardium may be as a result of the radiation she received 5 years ago. Do we have old CT's? Maybe this has been there for years and represents the pull-through in conjunction with the XRT. So I will guess that some is GI tract/stomach and the pleural effusion is chronic.
Maybe I'll turn out to be wrong but that's ok.
Actually, as I said before, this is not contrast in the GI tract. It is IV contrast, and all of the pathology is in the chest. Previous recent CT scans have shown a small effusion and she has had known pericardial effusions, but this is all new over about 3 months.
oops I didn't see your comment saying that that was IV, not oral contrast. Is that the atrium?
The contrast seen is in the right ventricle and, I believe, the right atrium.
How about an echo?
Several echocardiograms were done. Depending on who looked at it, the description varied from "pericardial mass compressing the left ventricle" to "extrinsic compression of the left ventricle." One echo referred to the left ventricle as "slit like" and all echos described "constrictive physiology."
If there are no other comments, I'll close this out tomorrow. Other than an echo, no one has suggested any diagnostic/therapeutic approach...
MRIs are not as widely used for chest imaging as CTs but in this case it might be an alternative. An MR with MRA of the chest might provide better tissue differentiation and identify the blood supply (and origin) of the various structures on that CT.
Yep, and it did. Initially, the cardiac surgeons said it was in the lung, and the thoracic surgeon said it was a consequence of her radiation treatment (he had evaluated this entire field a few months earlier, and he could not belive that it could be tumor).
Interventional radiology was able to aspirate 3 cc's, and thought it was a hematoma. Eventually an MRI showed that this lesion was invading the pericardium.
She was taken to the OR for exploration, which turned out to be an open and close procedure, as her entire left hemithorax and pericardium was tumor. She was discharged to hospice care.
Take home- if it doesn't look like an abscess, look for another explanation before presuming it's an abscess.
Post a Commenttest post a comment